

Application of structured statistical analyses to identify a biomarker predictive of enhanced tralokinumab efficacy in phase III clinical trials for severe, uncontrolled asthma
- PMID: 31315668
- PMCID: PMC6637533
- DOI: 10.1186/s12890-019-0889-4
Application of structured statistical analyses to identify a biomarker predictive of enhanced tralokinumab efficacy in phase III clinical trials for severe, uncontrolled asthma
Abstract
Background: Tralokinumab is an anti-interleukin (IL)-13 monoclonal antibody investigated for the treatment of severe, uncontrolled asthma in two Phase III clinical trials, STRATOS 1 and 2. The STRATOS 1 biomarker analysis plan was developed to identify biomarker(s) indicative of IL-13 activation likely to predict tralokinumab efficacy and define a population in which there was an enhanced treatment effect; this defined population was then tested in STRATOS 2.
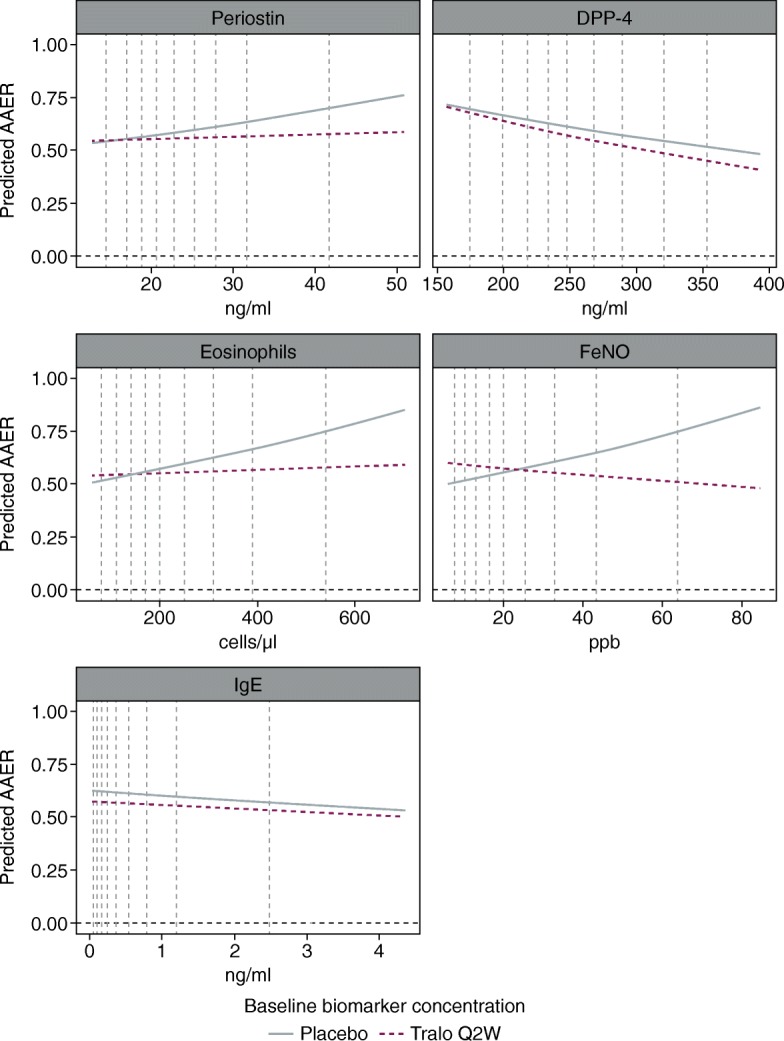
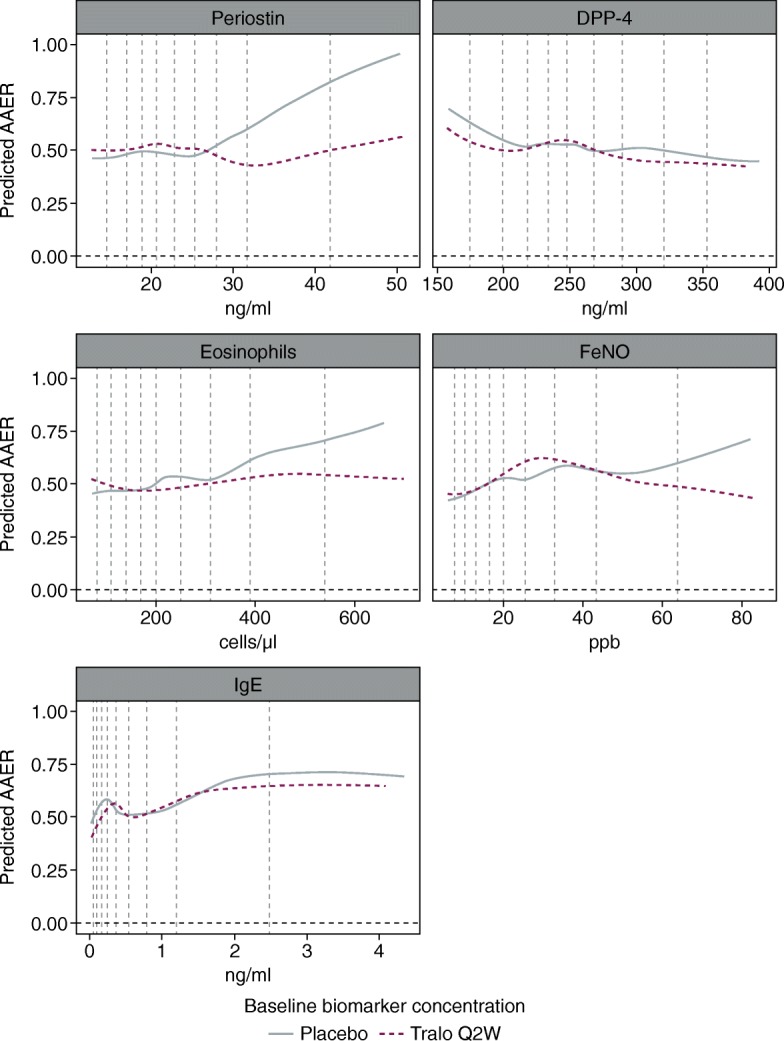
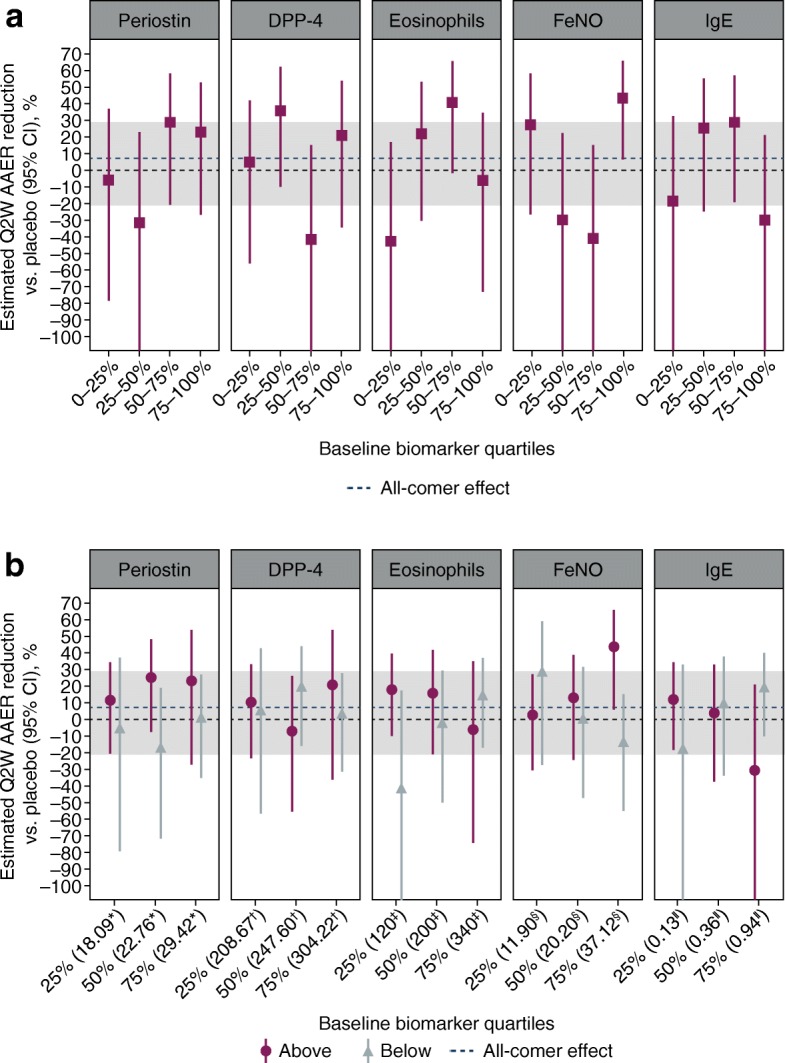
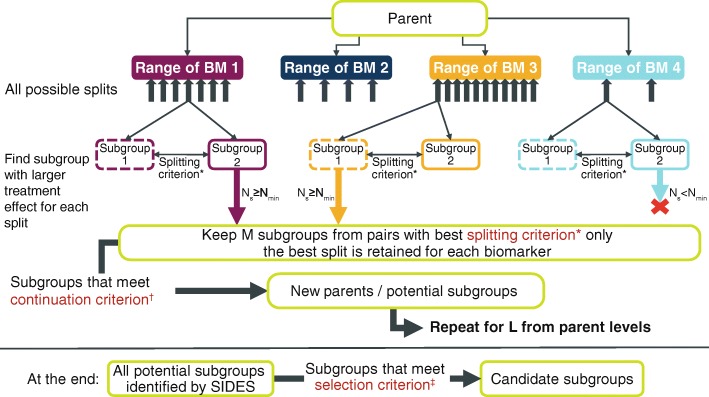
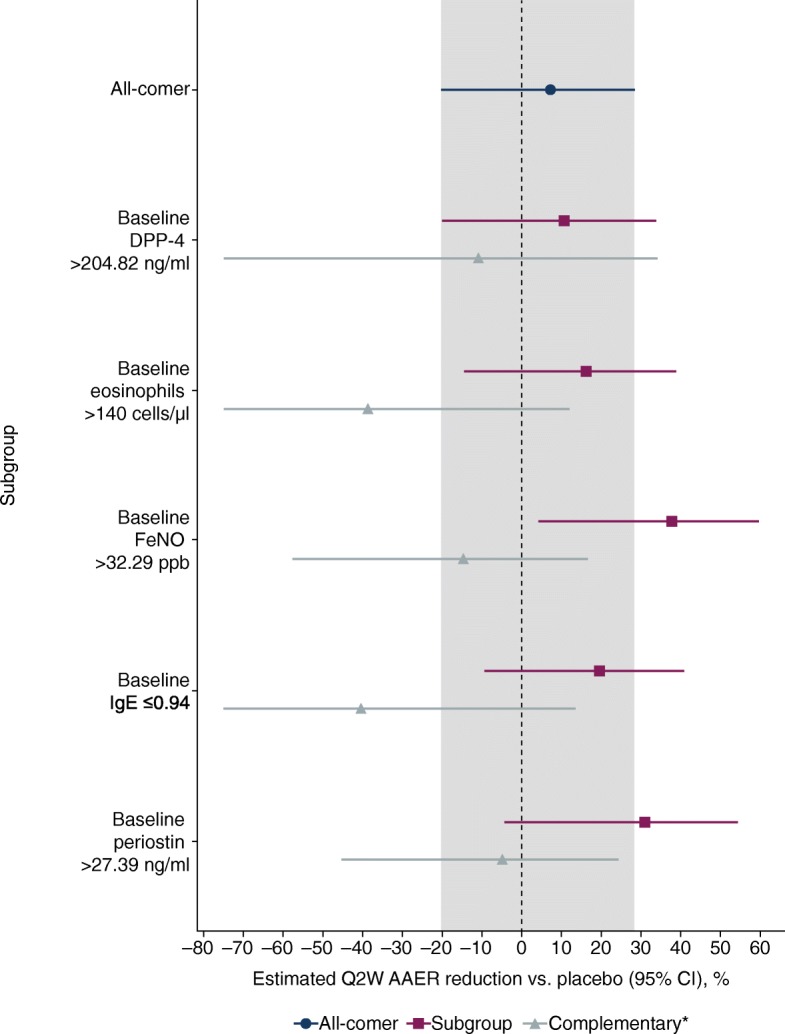
Methods: The biomarkers considered were blood eosinophil counts, fractional exhaled nitric oxide (FeNO), serum dipeptidyl peptidase-4, serum periostin and total serum immunoglobulin E. Tralokinumab efficacy was measured as the reduction in annualised asthma exacerbation rate (AAER) compared with placebo (primary endpoint measure of STRATOS 1 and 2). The biomarker analysis plan included negative binomial and generalised additive models, and the Subgroup Identification based on Differential Effect Search (SIDES) algorithm, supported by robustness and sensitivity checks. Effects on the key secondary endpoints of STRATOS 1 and 2, which included changes from baseline in standard measures of asthma outcomes, were also investigated. Prior to the STRATOS 1 read-out, numerous simulations of the methodology were performed with hypothetical data.
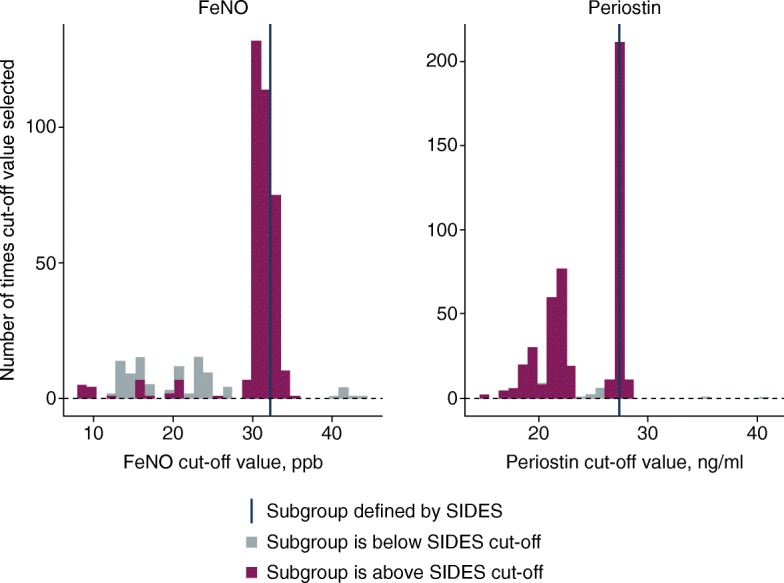
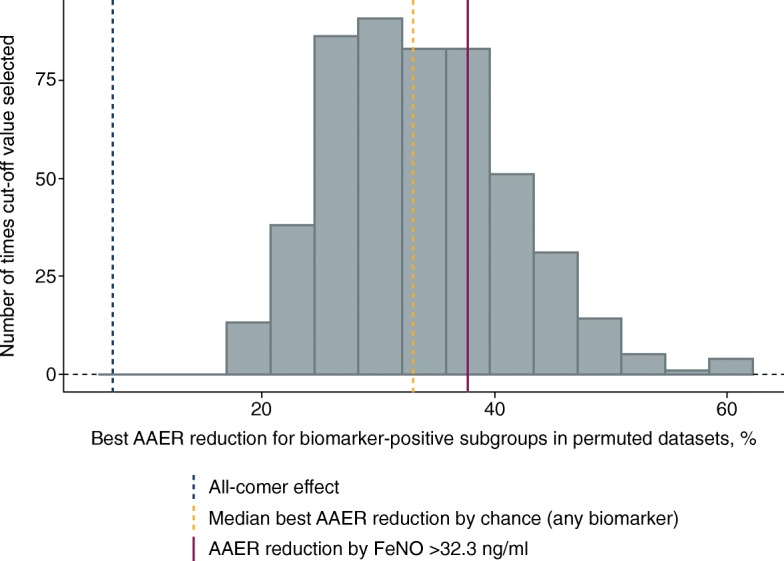
Results: FeNO and periostin were identified as the only biomarkers potentially predictive of treatment effect, with cut-offs chosen by the SIDES algorithm of > 32.3 ppb and > 27.4 ng/ml, respectively. The FeNO > 32.3 ppb subgroup was associated with greater AAER reductions and improvements in key secondary endpoints compared with the periostin > 27.4 ng/ml subgroup. Upon further evaluation of AAER reductions at different FeNO cut-offs, ≥37 ppb was chosen as the best cut-off for predicting tralokinumab efficacy.
Discussion: A rigorous statistical approach incorporating multiple methods was used to investigate the predictive properties of five potential biomarkers and to identify a participant subgroup that demonstrated an enhanced tralokinumab treatment effect. Using STRATOS 1 data, our analyses identified FeNO at a cut-off of ≥37 ppb as the best assessed biomarker for predicting enhanced treatment effect to be tested in STRATOS 2. Our findings were inconclusive, which reflects the complexity of subgroup identification in the severe asthma population.
Trial registration: STRATOS 1 and 2 are registered on ClinicalTrials.gov ( NCT02161757 registered on June 12, 2014, and NCT02194699 registered on July 18, 2014).
Keywords: Asthma; IL-13; Predictive biomarker; SIDES (subgroup identification based on differential effect search); STRATOS 1; STRATOS 2; Subgroup identification; Tralokinumab (up to 10).
Conflict of interest statement
MG, DJS, MH, KB, PW and GC are all employees of AstraZeneca, the sponsor of STRATOS 1 and STRATOS 2, and KB owns AstraZeneca shares. IL was an employee of IQVIA (formerly Quintiles) at the time of the study and provided consulting services per AstraZeneca’s contract with Quintiles; he is currently an employee of Eli Lilly.
Figures

References
-
- Zhu Z, Homer RJ, Wang Z, Chen Q, Geba GP, Wang J, Zhang Y, Elias JA. Pulmonary expression of interleukin-13 causes inflammation, mucus hypersecretion, subepithelial fibrosis, physiologic abnormalities, and eotaxin production. J Clin Invest. 1999;103:779–788. doi: 10.1172/JCI5909. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
