

A multimodality test to guide the management of patients with a pancreatic cyst
- PMID: 31316009
- PMCID: PMC7859881
- DOI: 10.1126/scitranslmed.aav4772
A multimodality test to guide the management of patients with a pancreatic cyst
Abstract
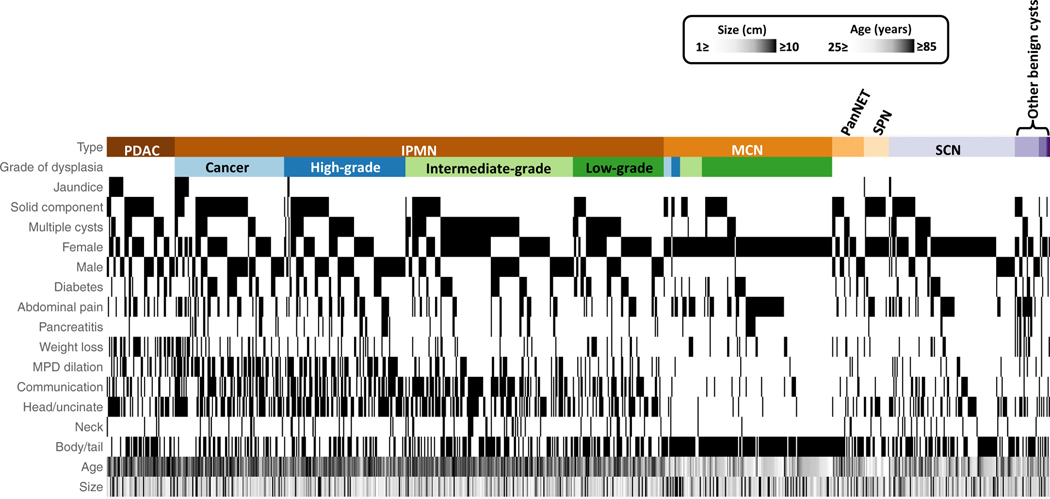
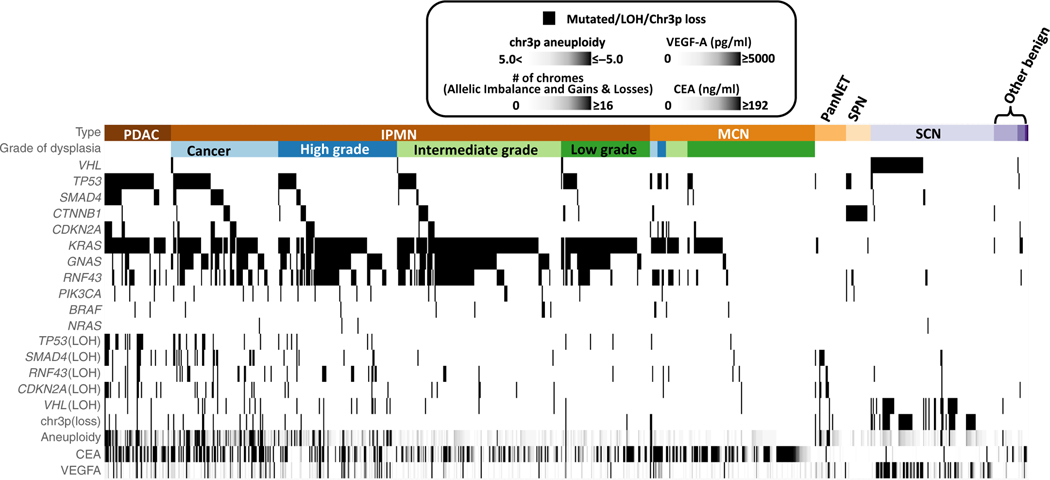
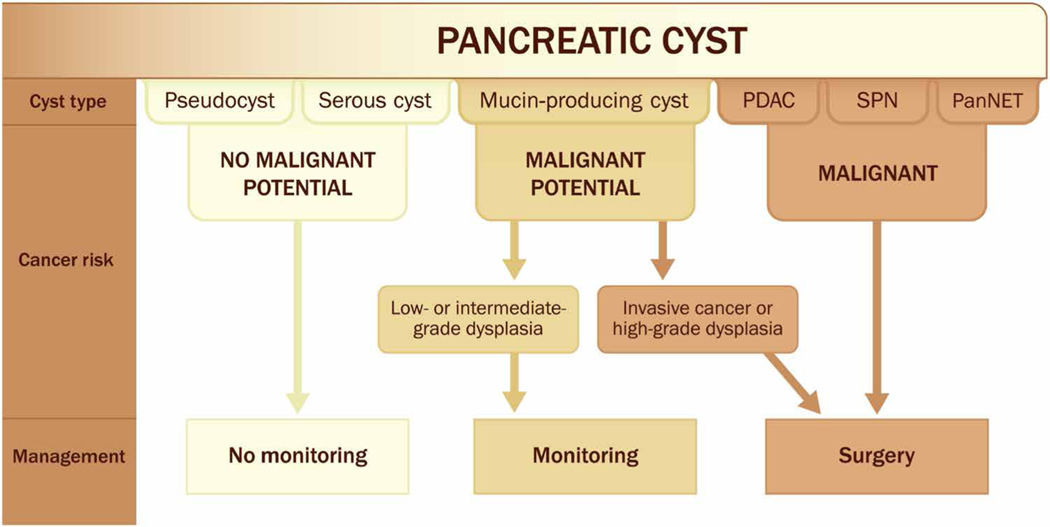
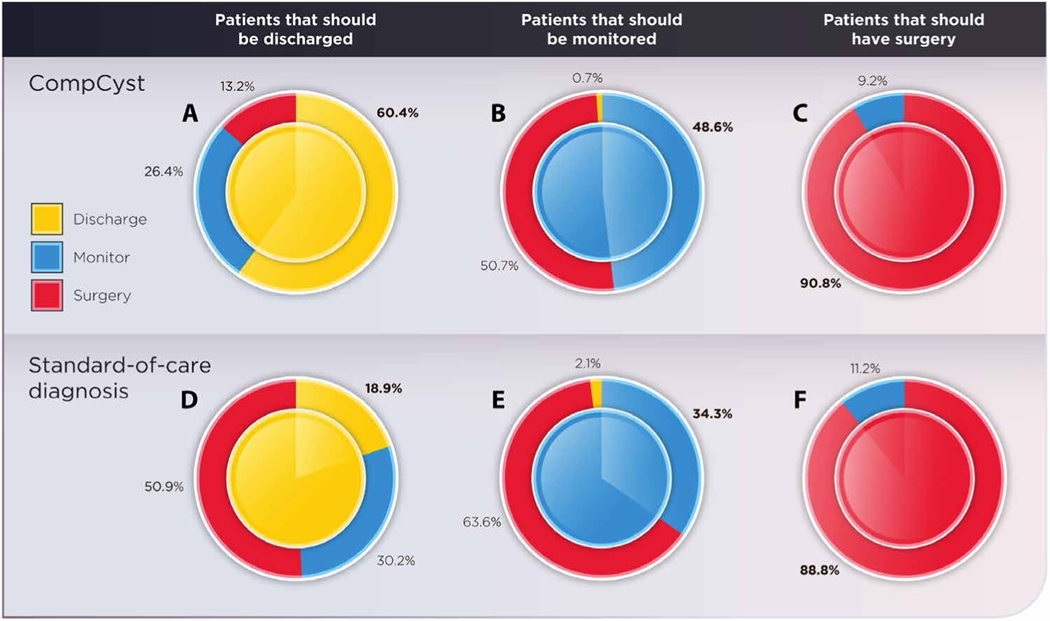
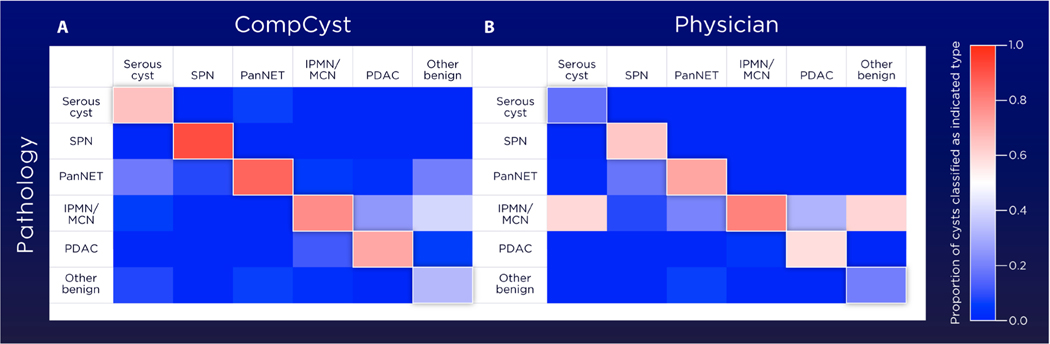
Pancreatic cysts are common and often pose a management dilemma, because some cysts are precancerous, whereas others have little risk of developing into invasive cancers. We used supervised machine learning techniques to develop a comprehensive test, CompCyst, to guide the management of patients with pancreatic cysts. The test is based on selected clinical features, imaging characteristics, and cyst fluid genetic and biochemical markers. Using data from 436 patients with pancreatic cysts, we trained CompCyst to classify patients as those who required surgery, those who should be routinely monitored, and those who did not require further surveillance. We then tested CompCyst in an independent cohort of 426 patients, with histopathology used as the gold standard. We found that clinical management informed by the CompCyst test was more accurate than the management dictated by conventional clinical and imaging criteria alone. Application of the CompCyst test would have spared surgery in more than half of the patients who underwent unnecessary resection of their cysts. CompCyst therefore has the potential to reduce the patient morbidity and economic costs associated with current standard-of-care pancreatic cyst management practices.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
Guiding pancreatic cyst management.Nat Rev Gastroenterol Hepatol. 2019 Oct;16(10):582-583. doi: 10.1038/s41575-019-0198-7. Nat Rev Gastroenterol Hepatol. 2019. PMID: 31409907 No abstract available.
References
-
- Lee KS, Sekhar A, Rofsky NM, Pedrosa I, Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am. J. Gastroenterol 105, 2079–2084 (2010). - PubMed
-
- Lennon AM, Wolfgang CL, Canto MI, Klein AP, Herman JM, Goggins M,Fishman EK, Kamel I, Weiss MJ, Diaz LA, Papadopoulos N, Kinzler KW,Vogelstein B, Hruban RH, The early detection of pancreatic cancer: What will it take to diagnose and treat curable pancreatic neoplasia? Cancer Res. 74,3381–3389 (2014). - PMC - PubMed
-
- Tanaka M, Fernández-del Castillo C, Kamisawa T, Jang JY, Levy P, Ohtsuka T, Salvia R,Shimizu Y, Tada M, Wolfgang CL, Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 17, 738–753 (2017). - PubMed
-
- Del Chiaro M, Verbeke C, Salvia R, Klöppel G, Werner J, McKay C, Friess H, Manfredi R,Van Cutsem E, Löhr M, Segersvärd R; European Study Group on Cystic Tumours of the Pancreas, European experts consensus statement on cystic tumours of the pancreas. Dig. Liver Dis 45, 703–711 (2013). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
