

Effect of Home-Based High-Intensity Interval Training in Patients With Lacunar Stroke: A Randomized Controlled Trial
- PMID: 31316451
- PMCID: PMC6611174
- DOI: 10.3389/fneur.2019.00664
Effect of Home-Based High-Intensity Interval Training in Patients With Lacunar Stroke: A Randomized Controlled Trial
Abstract
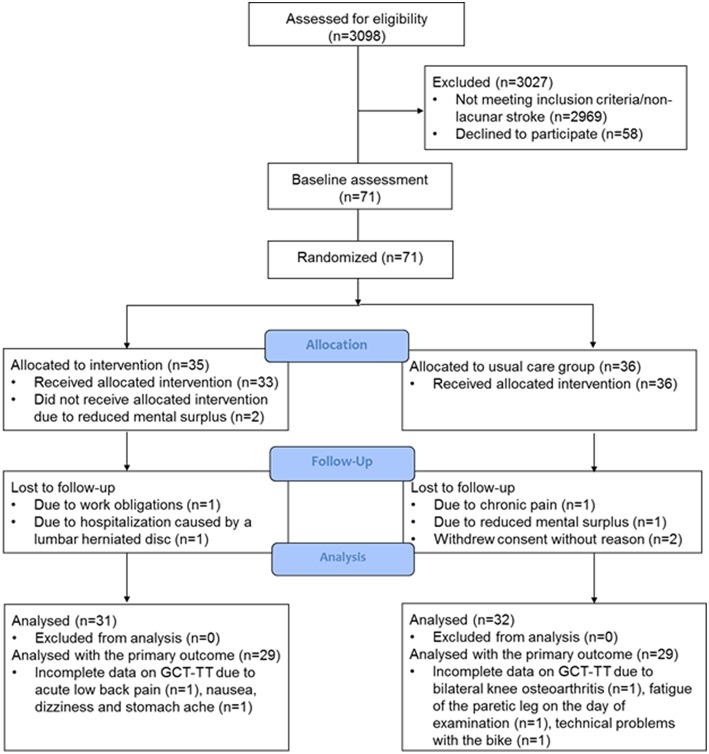
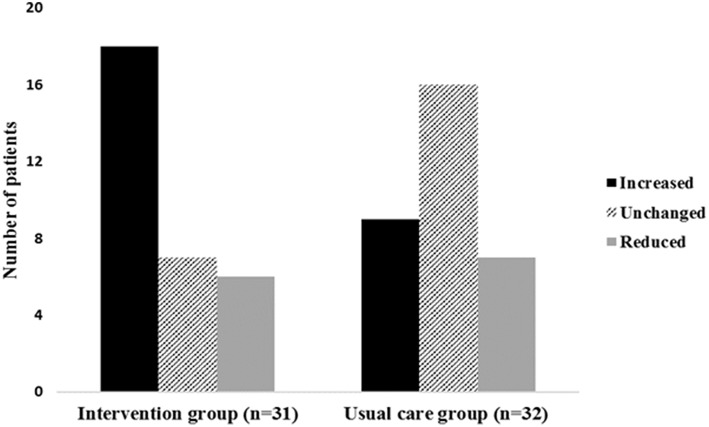
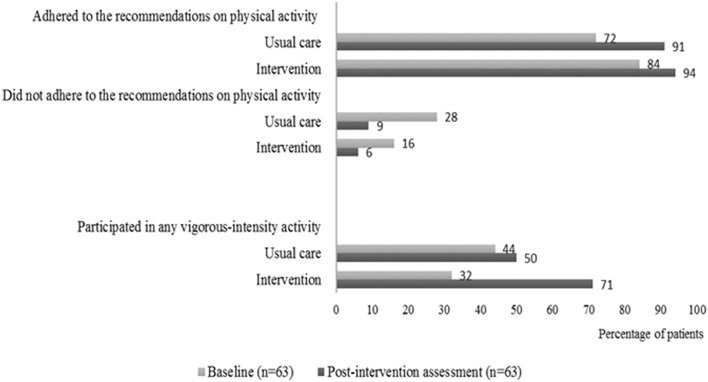
Background: High-intensity interval training (HIIT) is superior to moderate-intensity continuous training in improving cardiorespiratory fitness in patients with cardiovascular disease, but is it safe, feasible and effective in patients with stroke? We investigated feasibility and effect of early, home-based HIIT in patients with lacunar stroke combined with usual care vs. usual care, only. Methods: Patients with minor stroke (severity: 55/58 point on the Scandinavian Stroke Scale) were randomized to HIIT or usual care in a randomized, controlled trial. We measured the following outcomes at baseline and post-intervention: cardiorespiratory fitness monitored as power output from the Graded Cycling Test with Talk Test (GCT-TT; primary outcome), physical activity, fatigue, depression, well-being, stress, cognition, endothelial function, blood pressure, body mass index, and biomarkers. Results: We included 71 patients (mean age 63.7 ± 9.2), 49 men, 31 in intervention group. Home-based HIIT was feasible with no reported adverse events in relation to the intervention. No significant change between the groups in GCT-TT power output was detected (p = 0.90). The change in time spent on vigorous-intensity activity was 2 h/week and 0.6 h/week, intervention and usual care, respectively (p = 0.045). There were no significant differences between groups in the remaining secondary outcomes. Conclusion: HIIT was feasible and safe in patients with lacunar stroke. Patients can engage early in home-based HIIT when involved in choosing exercise modality and guided by weekly motivational phone calls. Within 3 months, HIIT did, however, not yield effect on cardiorespiratory fitness. We await further evaluation of long-term effects of this intervention on continued regular physical exercise and cardiovascular event. Clinical Trial Registration: https://clinicaltrials.gov, identifier NCT02731235.
Keywords: aerobic exercise; high-intensity interval training; home-based physical activity; lacunar stroke; secondary stroke prevention.
Figures
Comment in
-
Physical fitness training after stroke-a crucial and exciting field for service development and research.J Stroke Cerebrovasc Dis. 2023 Apr;32(4):106991. doi: 10.1016/j.jstrokecerebrovasdis.2023.106991. Epub 2023 Jan 25. J Stroke Cerebrovasc Dis. 2023. PMID: 36707269 No abstract available.
References
Associated data
LinkOut - more resources
Full Text Sources
Medical