

Evaluation and Management of Angioedema in the Emergency Department
- PMID: 31316698
- PMCID: PMC6625683
- DOI: 10.5811/westjem.2019.5.42650
Evaluation and Management of Angioedema in the Emergency Department
Abstract
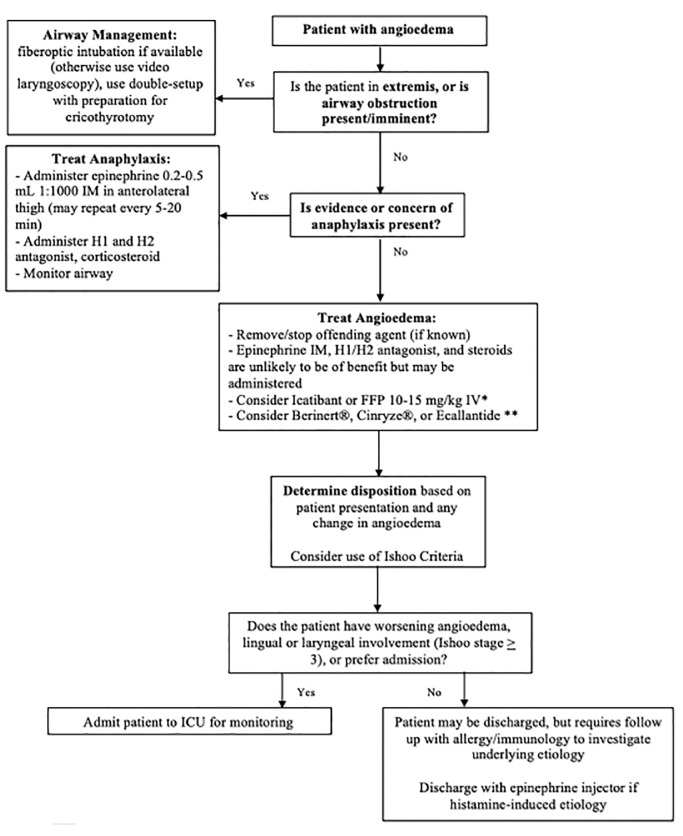
Angioedema is defined by non-dependent, non-pitting edema that affects several different sites and is potentially life-threatening due to laryngeal edema. This narrative review provides emergency physicians with a focused overview of the evaluation and management of angioedema. Two primary forms include histamine-mediated and bradykinin-mediated angioedema. Histamine-mediated forms present similarly to anaphylaxis, while bradykinin-mediated angioedema presents with greater face and oropharyngeal involvement and higher risk of progression. Initial evaluation and management should focus on evaluation of the airway, followed by obtaining relevant historical features, including family history, medications, and prior episodes. Histamine-mediated angioedema should be treated with epinephrine intramuscularly, antihistaminergic medications, and steroids. These medications are not effective for bradykinin-mediated forms. Other medications include C1-INH protein replacement, kallikrein inhibitor, and bradykinin receptor antagonists. Evidence is controversial concerning the efficacy of these medications in an acute episode, and airway management is the most important intervention when indicated. Airway intervention may require fiberoptic or video laryngoscopy, with preparation for cricothyrotomy. Disposition is dependent on patient's airway and respiratory status, as well as the sites involved.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. This review does not reflect the views or opinions of the U.S. government, Department of Defense, U.S. Army, U.S. Air Force, or SAUSHEC EM Residency Program. There are no conflicts of interest or sources of funding to declare.
Figures
References
-
- Bork K. An evidence based therapeutic approach to hereditary and acquired angioedema. Curr Opin Allergy Clin Immunol. 2014;14(4):354–62. - PubMed
-
- Bork K. Angioedema. Immunol Allergy Clin North Am. 2014;34(1):23–31. - PubMed
-
- Wilkerson RG. Angioedema in the emergency department: an evidence-based review. Emerg Med Pract. 2012;14(11):1–21. - PubMed
-
- Frigas E, Nzeako UC. Angioedema. Pathogenesis, differential diagnosis, and treatment. Clin Rev Allergy Immunol. 2002;23(2):217–3. - PubMed