

Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Posterior Petrosal Approach
- PMID: 31316880
- PMCID: PMC6635129
- DOI: 10.1055/s-0038-1675174
Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Posterior Petrosal Approach
Abstract
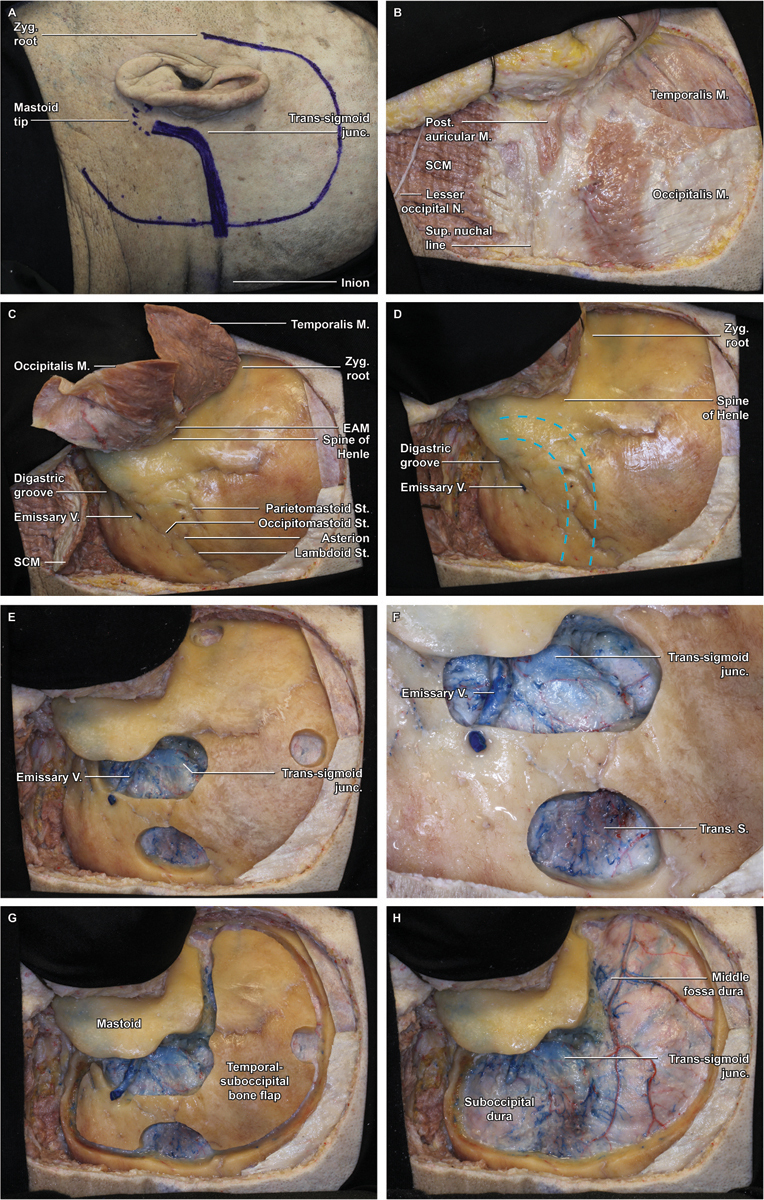
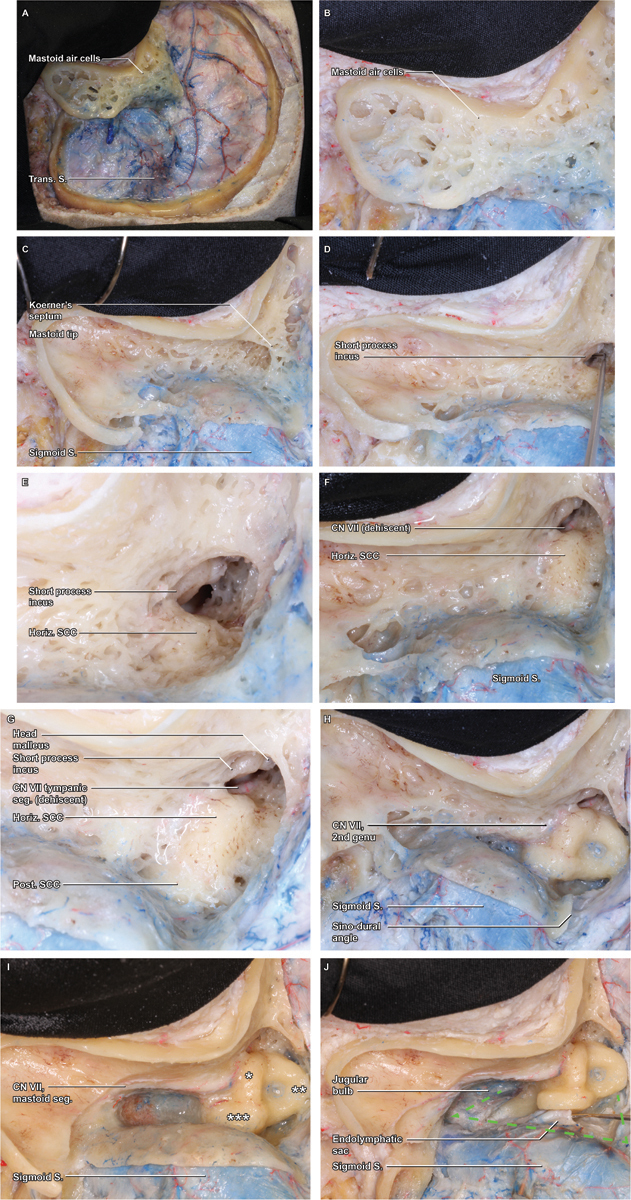
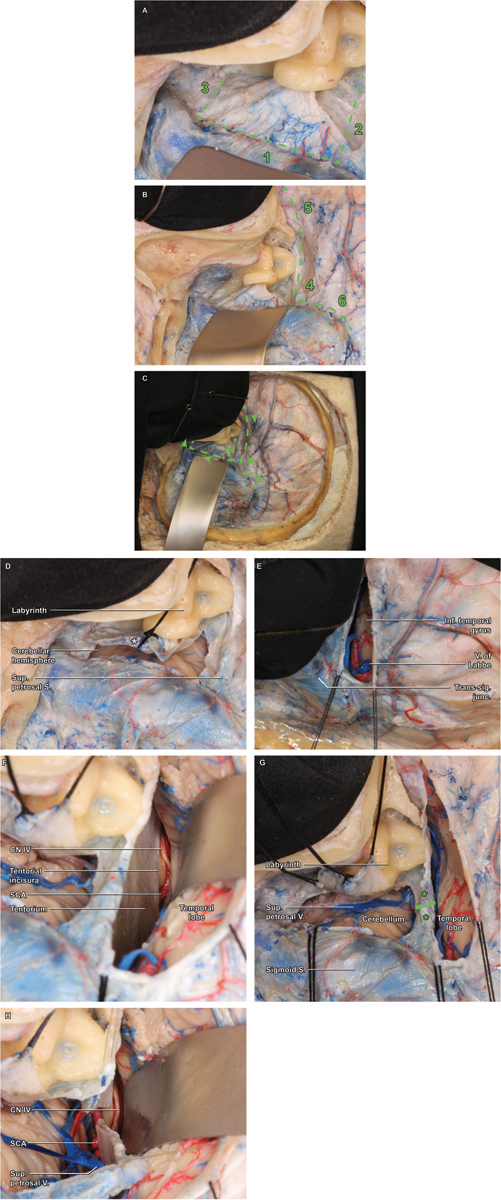
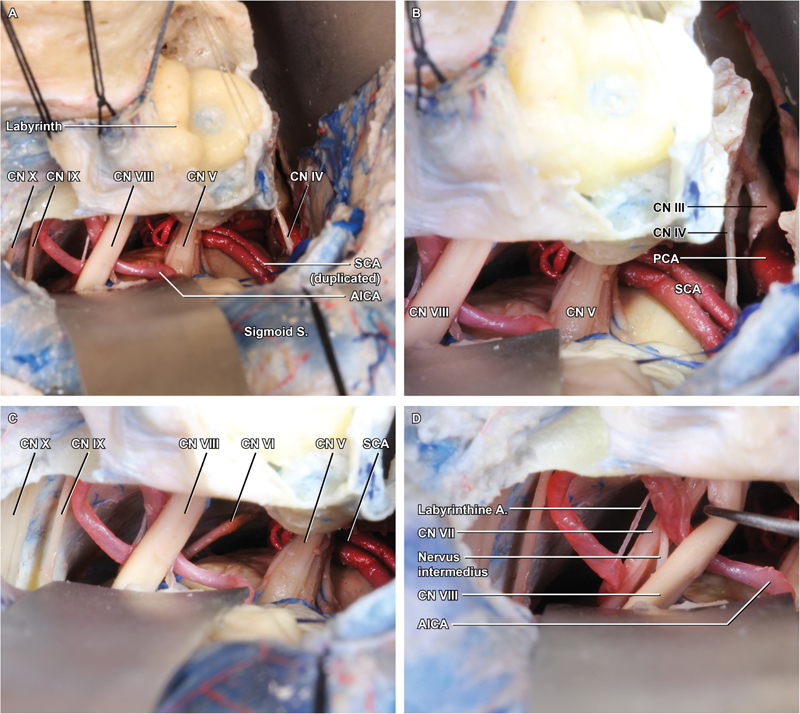
Introduction Although numerous anatomical and operative atlases have been published, those that have focused on the skull base either have provided views that are quite difficult to achieve in the operating room to better depict surgical anatomy or are written at the level of an audience with considerable knowledge and experience. Methods Five sides of three formalin-fixed latex-injected specimens were dissected under microscopic magnification. A posterior petrosectomy approach was performed by three neurosurgical residents at different training levels with limited previous experience in anatomical dissection mentored by the senior authors (C. L. W. D. and M. J. L.) and a clinical skull base fellow with additional anatomical dissection experience (M. P. C.). Anatomical dissections were performed until the expected level of dissection quality was achieved to demonstrate each important step of the surgical approach that would be understandable to all trainees of all levels. Following dissection education, representative case applications were reviewed. Results The posterior petrosectomy (also known as presigmoid retrolabyrinthine approach) affords excellent access to cranial nerves III to XI and a diverse array of pathologies. Key steps include positioning and skin incision, scalp and muscle flaps, burr holes, craniotomy flap elevation, superficial mastoidectomy, otic capsule exposure and presigmoid dura decompression, primary presigmoid durotomy, inferior temporal durotomy, superior petrosal sinus ligation, tentorium sectioning, and final exposure. Conclusion The posterior petrosectomy is a challenging approach; thorough operative-style laboratory dissection is essential to provide trainees with a suitable guide. We describe a comprehensive approach to learning this technique, intended to be understandable and usable by a resident audience.
Keywords: brainstem; education; meningioma; posterior petrosectomy; skull base.
Conflict of interest statement
Figures
References
-
- Wanibuchi M, Friedmann A H, Fukushima T. Stuttgart: Thieme Medical Publishers; 2009. Photo Atlas of Skull Base Dissection: Techniques and Operative Approaches; p. 432.
-
- Tew J M, van Loveren H R, Keller J T. London: WB Saunders Co. Ltd; 2001. Atlas of Operative Microneurosurgery: Brain Tumors v. 2; p. 446.
-
- Bambakidis N C, Kakarla U K, Kim L Jet al. Evolution of surgical approaches in the treatment of petroclival meningiomas: a retrospective review Neurosurgery 2007610502202–209., discussion 209–211 - PubMed
-
- Daspit C P, Spetzler R F, Pappas C T. Combined approach for lesions involving the cerebellopontine angle and skull base: experience with 20 cases--preliminary report. Otolaryngol Head Neck Surg. 1991;105(06):788–796. - PubMed
-
- Samii M, Ammirati M.The combined supra-infratentorial pre-sigmoid sinus avenue to the petro-clival region. Surgical technique and clinical applications Acta Neurochir (Wien) 198895(1-2):6–12. - PubMed
LinkOut - more resources
Full Text Sources
