

Successful therapy for autoimmune myocarditis with pembrolizumab treatment for nasopharyngeal carcinoma
- PMID: 31317017
- PMCID: PMC6603355
- DOI: 10.21037/atm.2019.04.73
Successful therapy for autoimmune myocarditis with pembrolizumab treatment for nasopharyngeal carcinoma
Abstract
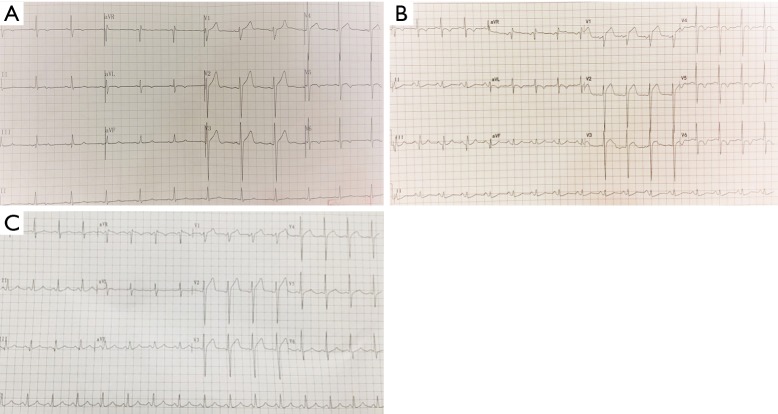
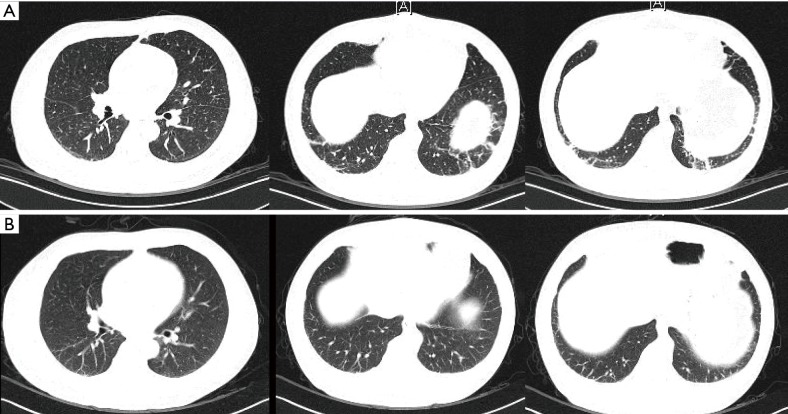
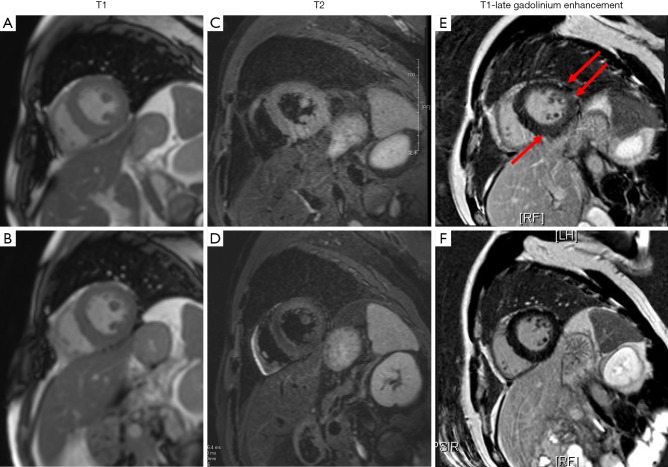
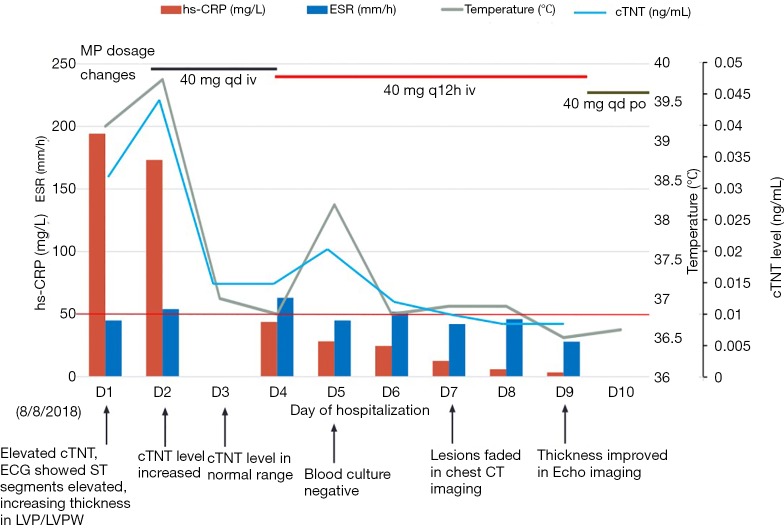
Immune checkpoint inhibitors (ICIs), including inhibitors of cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4), programmed death-1 (PD-1) and programmed death-ligand 1 (PD-L1) have demonstrated prominent clinical benefits in a variety of cancers and have been rapidly applied to treat a variety of carcinomas such as melanoma, non-small-cell lung cancer, and head and neck cancer. Meanwhile, the occurrence of immune-related adverse events (irAEs) has been increasing. In this case, we report a 45-year-old man with metastatic nasopharyngeal carcinoma suffering from pulmonary fibrosis and myocarditis on the 4th day after receiving pembrolizumab treatment which belongs to anti-PD-1 drugs. Although the endomyocardial biopsy (EMB) could not be performed, the strong temporal association with pembrolizumab treatment and the specific changes of electrocardiograph, echocardiography and cardiovascular magnetic resonance (CMR) suggest that the myocardial injury and edema were related to pembrolizumab-induced myocarditis. With glucocorticoid treatment, the symptoms and myocardium lesion were almost resolved and the patient agreed to tapered chemotherapy with steroid treatment.
Keywords: Fever; immune checkpoint inhibitors (ICIs); immune-related adverse events (irAEs).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials