

Intrafamilial Variability of ADPKD
- PMID: 31317121
- PMCID: PMC6611955
- DOI: 10.1016/j.ekir.2019.04.018
Intrafamilial Variability of ADPKD
Abstract
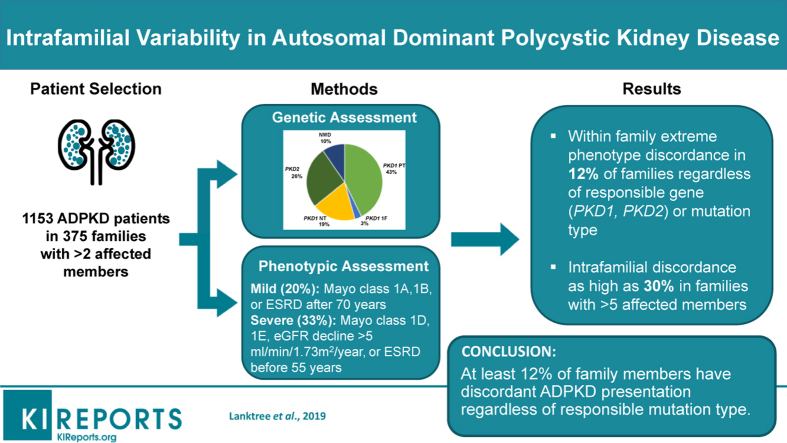
Introduction: Discordance in kidney disease severity between affected relatives is a recognized feature of autosomal dominant polycystic kidney disease (ADPKD). Here, we report a systematic study of a large cohort of families to define the prevalence and clinical features of intrafamilial discordance in ADPKD.
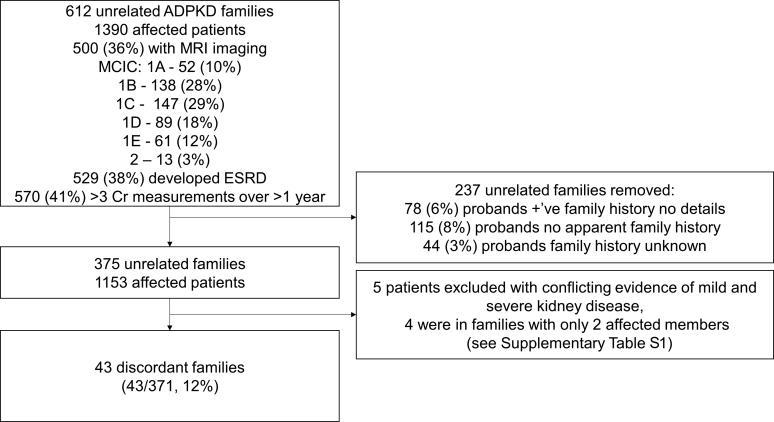
Methods: The extended Toronto Genetic Epidemiology Study of Polycystic Kidney Disease (eTGESP) cohort includes 1390 patients from 612 unrelated families with ADPKD ascertained in a regional polycystic kidney disease center. All probands underwent comprehensive PKD1 and PKD2 mutation screening. Total kidney volume by magnetic resonance imaging (MRI) was available in 500 study patients.
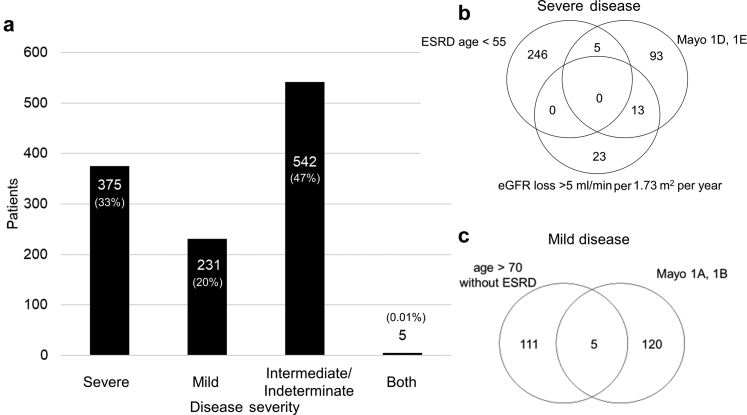
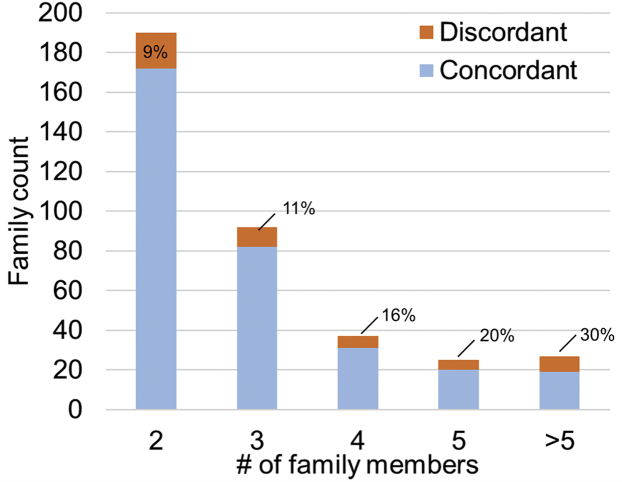
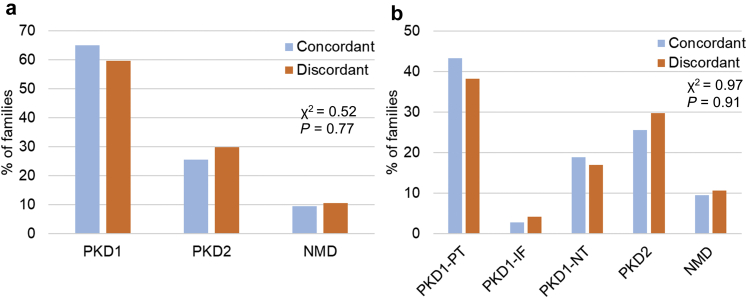
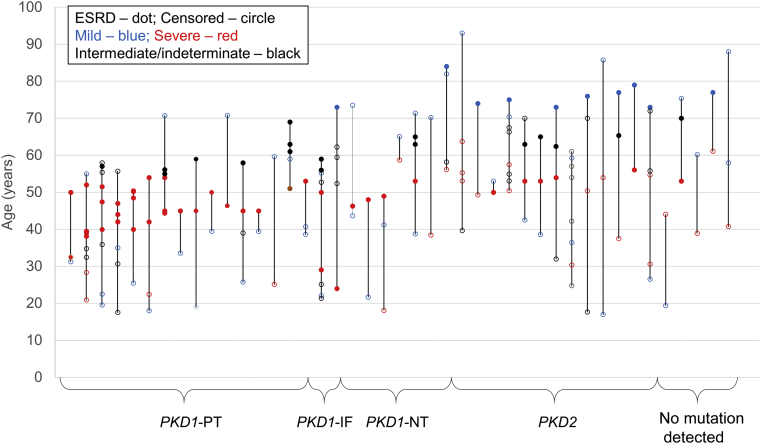
Results: Based on (i) rate of estimated glomerular filtration rate (eGFR) decline, (ii) age at onset of end-stage renal disease (ESRD), and (iii) Mayo Clinic Imaging Classification (MCIC), 20% of patients were classified as having mild disease, and 33% as having severe disease. Intrafamilial ADPKD discordance with at least 1 mild and 1 severe case was observed in 43 of 371 (12%) families, at a similar frequency regardless of the responsible gene (PKD1/PKD2/no mutation detected) or mutation type (protein-truncating versus nontruncating). Intrafamilial discordance was more common in larger families and was present in 30% of families with more than 5 affected members. The heritability of age at onset of ESRD was similar between different mutation types.
Conclusion: Extreme kidney disease discordance is present in at least 12% of families with ADPKD, regardless of the underlying mutated gene or mutation class. Delineating genetic and environmental modifiers underlying the observed intrafamilial ADPKD variability will provide novel insights into the mechanisms of progression in ADPKD.
Keywords: ADPKD; genetics; polycystic kidney disease.
Figures
References
-
- Spithoven E.M., Kramer A., Meijer E. Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival─an analysis of data from the ERA-EDTA Registry. Nephrol Dial Transplant. 2014;29(suppl 4):iv15–iv25. - PMC - PubMed
- Spithoven EM, Kramer A, Meijer E, et al. Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival─an analysis of data from the ERA-EDTA Registry. Nephrol Dial Transplant. 2014;29(suppl 4):iv15-iv25. - PMC - PubMed
-
- Torres V.E., Chapman A.B., Devuyst O. Tolvaptan in later-stage autosomal dominant polycystic kidney disease. N Engl J Med. 2017;377:1930–1942. - PubMed
- Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in later-stage autosomal dominant polycystic kidney disease. N Engl J Med. 2017;377:1930-1942. - PubMed
-
- Torres V.E., Chapman A.B., Devuyst O. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367:2407–2418. - PMC - PubMed
- Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367:2407-2418. - PMC - PubMed
-
- Barua M., Cil O., Paterson A.D. Family history of renal disease severity predicts the mutated gene in ADPKD. J Am Soc Nephrol. 2009;20:1833–1838. - PMC - PubMed
- Barua M, Cil O, Paterson AD, et al. Family history of renal disease severity predicts the mutated gene in ADPKD. J Am Soc Nephrol. 2009;20:1833-1838. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
