

Implications of Left Bundle Branch Block in Takotsubo Cardiomyopathy: Propensity Match Analysis from the National Inpatient Sample
- PMID: 31317468
- PMCID: PMC6828991
- DOI: 10.1007/s40119-019-0141-6
Implications of Left Bundle Branch Block in Takotsubo Cardiomyopathy: Propensity Match Analysis from the National Inpatient Sample
Abstract
Introduction: Takotsubo cardiomyopathy (TTC), also called stress cardiomyopathy, is a transient reversible left ventricular dysfunction mimicking acute coronary syndrome (ACS). Studies have shown similar rates of in-hospital complications in TTC and myocardial infarction (MI). Left bundle branch block (LBBB) is associated with increased mortality in patients with MI; however, similar studies comparing outcomes of TTC in the presence of LBBB are lacking.
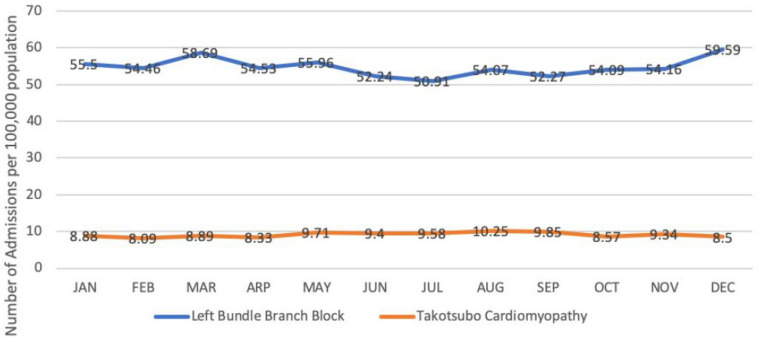
Methods: The 2016 National Inpatient Sample (NIS) database was queried to identify all admissions with a primary discharge diagnosis of TTC. Diagnosis-specific codes were used to stratify patients based on the presence or absence of LBBB. Both population sets were paired using 1:10 propensity score matching. Multivariate logistic regression analysis was performed to compare various in-hospital outcomes among both groups.
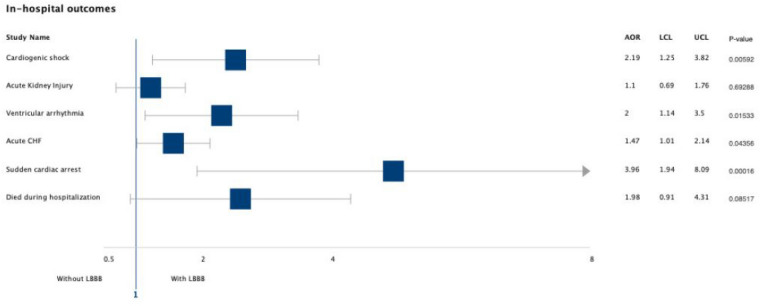
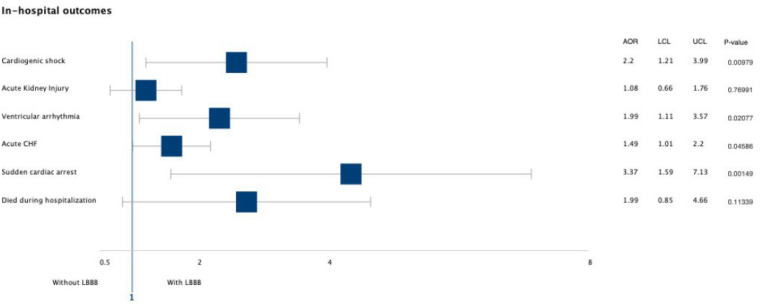
Results: Amongst 7270 admissions for TTC, 226 patients had concomitant LBBB. After performing 1:10 propensity matching, 130 patients with LBBB were compared to 1275 patients without LBBB. The presence of LBBB was associated with increased odds of cardiogenic shock (AOR = 2.2, 95% CI 1.21-3.99, p = 0.0097); ventricular arrhythmia (AOR 1.99, 95% CI 1.11-3.57, p = 0.02), acute congestive heart failure (AOR = 1.49, 95% CI 1.01-2.2, p = 0.04), and sudden cardiac arrest (AOR = 3.37, 95% CI 1.59-7.13, p = 0.0001). There was no statistical difference in all-cause in-hospital mortality, however a trend towards worsening was noted.
Conclusions: The incidence of arrhythmia and shock in patients with TTC does not correlate with the extent of myocardium involvement. The presence of LBBB in such cases can help recognize at-risk populations, and with timely intervention, life-threatening complications can be avoided. Despite limitations of the dataset and inability to establish causality, prospective studies with longer follow-up are warranted.
Keywords: Arrhythmia; Conduction disorders; Left bundle branch block; Stress cardiomyopathy; Takotsubo cardiomyopathy.
Conflict of interest statement
Dipesh Ludhwani, Mouyyad Rahaby, Vasu Patel, Saad Jamil, Adam Kedzia and Chunyi Wu have nothing to disclose.
Figures
References
-
- Dote K. Myocardial stunning due to simultaneous multivessel coronary spasm: a review of five cases. J Cardiol. 1991;21:203–214. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78–e140. doi: 10.1016/j.jacc.2012.11.019. - DOI - PubMed
LinkOut - more resources
Full Text Sources
