

Contemporary benefit-harm profile over two decades in primary prophylactic ICD-therapy
- PMID: 31317573
- PMCID: PMC6788478
- DOI: 10.1002/clc.23234
Contemporary benefit-harm profile over two decades in primary prophylactic ICD-therapy
Abstract
Background: Implantable cardioverter defibrillator (ICD) was implemented into clinical routine more than 20 years ago. Since then, ICD therapy became standard therapy for primary and secondary prevention of sudden cardiac death in clinical practice.
Objectives: Aim of the study was to evaluate the benefit-harm profile of contemporary primary prophylactic ICD therapy.
Methods: A total of 1222 consecutive patients of a prospective single-center ICD-registry were analyzed who underwent primary prophylactic ICD implantation between 2000 and 2017. Patients were divided into two groups according to the implantation year: 2010-2017 (group 1, n = 579) and 2000-2009 (group 2, n = 643).
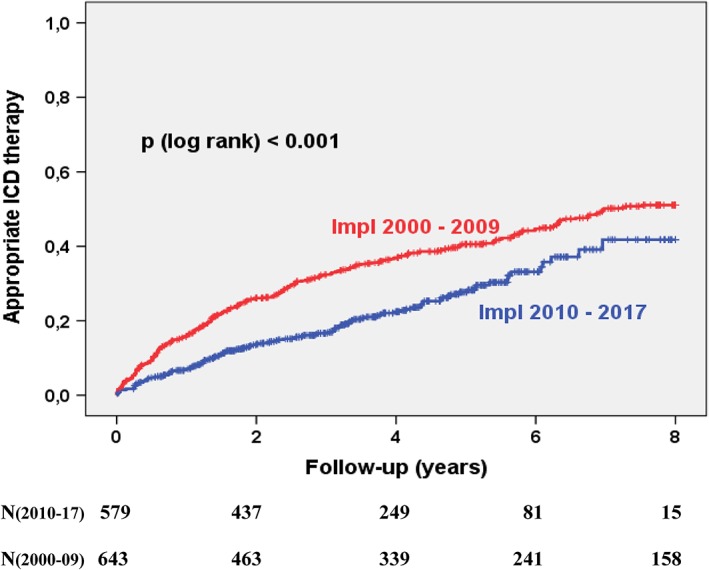
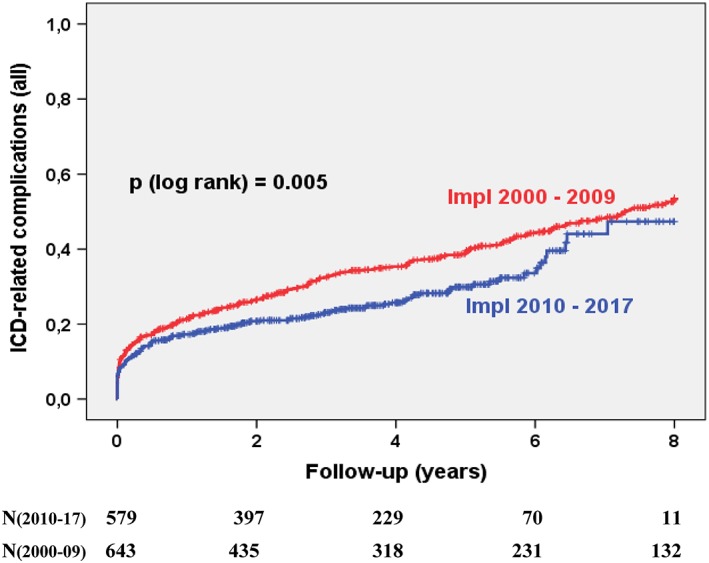
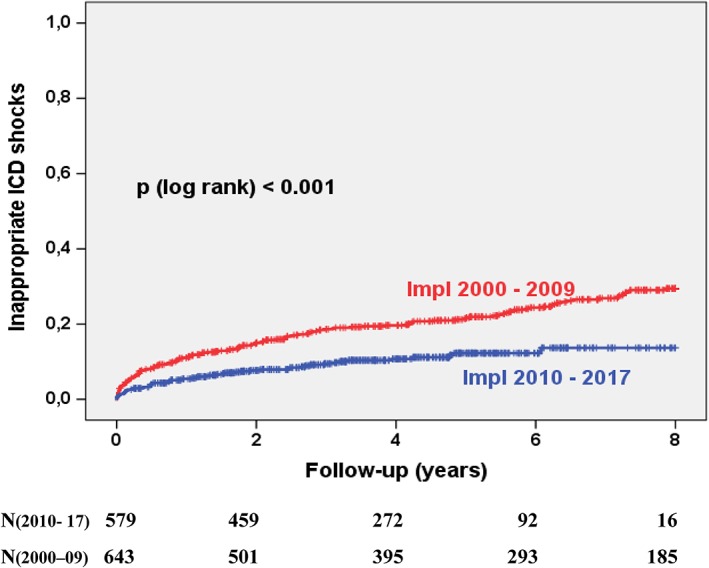
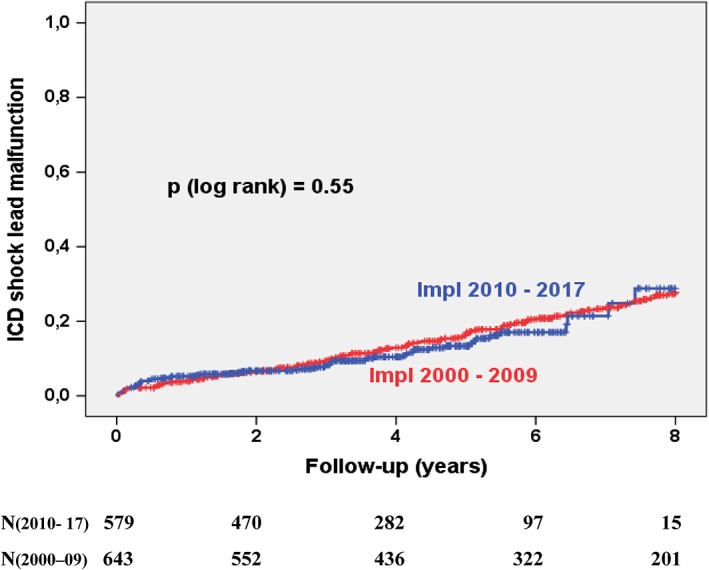
Results: The rate of estimated appropriate ICD therapy after 8 years was 51% in the 2000s and 42% in the 2010s (P < .001). The complication rate changed slightly from 53% to 47% (P = .005). This decline was mainly driven by the reduction of inappropriate ICD shocks (30% vs 14%, P < .001) whereas the rate of ICD shock lead malfunction and device/ lead infection remained unchanged over time. Nonischemic cardiomyopathy was an independent predictor for ICD complications without benefit of ICD therapy (HR 1.37, 95% CI 1.07-1.77).
Conclusion: The ICD therapy rate for ventricular arrhythmias in patients with primary prophylactic ICD implantation is decreasing over the last two decades. Complication rate remains high due to an unchanged rate of ICD shock malfunctions and device infections. Nonischemic cardiomyopathy is an independent predictor for ICD complications without benefit of ICD therapy in primary prophylactic ICD-therapy.
Keywords: ICD complications; ICD shock; defibrillation; implantable cardioverter defibrillator (ICD); primary prophylactic ICD.
© 2019 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflict of interests.
Figures
References
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877‐883. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter‐defibrillator for congestive heart failure. N Engl J Med. 2005;352:225‐237. - PubMed
-
- Maggioni AP, Anker SD, Dahlström U, et al. Are hospitalized or ambulatory patients with heart failure treated in accordance with European Society of Cardiology guidelines? Evidence from 12,440 patients of the ESC heart failure long‐term registry. Eur J Heart Fail. 2013;15:1173‐1184. - PubMed
-
- Raatikainen MJ, Arnar DO, Zeppenfeld K, Merino JL, Kuck KH, Hindricks G. Current trends in the use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology member countries: 2015 report from the European heart rhythm association. Europace. 2015;17(Suppl 4):iv1‐iv72. - PubMed
-
- Køber L, Thune JJ, Nielsen JC, et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016;375:1221‐1230. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
