

Invasive and antiplatelet treatment of patients with non-ST-segment elevation myocardial infarction: Understanding and addressing the global risk-treatment paradox
- PMID: 31317575
- PMCID: PMC6788484
- DOI: 10.1002/clc.23232
Invasive and antiplatelet treatment of patients with non-ST-segment elevation myocardial infarction: Understanding and addressing the global risk-treatment paradox
Abstract
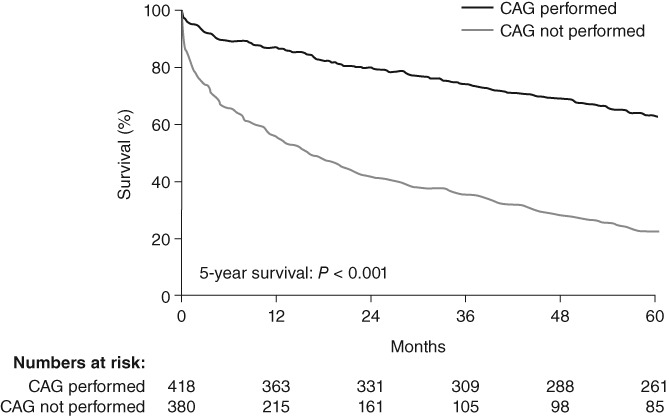
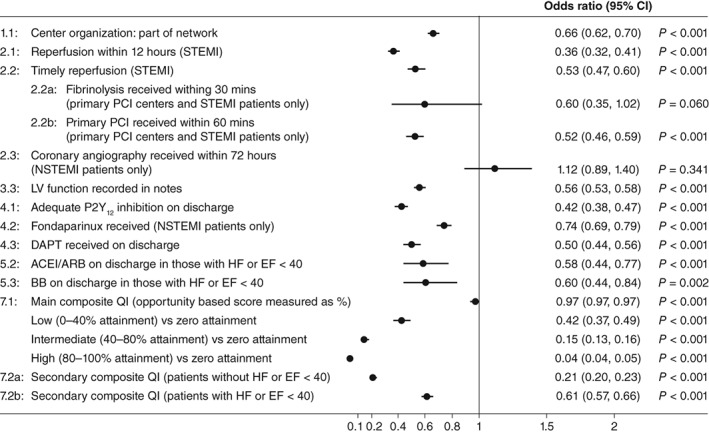
Clinical guidelines for the treatment of patients with non-ST-segment elevation myocardial infarction (NSTEMI) recommend an invasive strategy with cardiac catheterization, revascularization when clinically appropriate, and initiation of dual antiplatelet therapy regardless of whether the patient receives revascularization. However, although patients with NSTEMI have a higher long-term mortality risk than patients with ST-segment elevation myocardial infarction (STEMI), they are often treated less aggressively; with those who have the highest ischemic risk often receiving the least aggressive treatment (the "treatment-risk paradox"). Here, using evidence gathered from across the world, we examine some reasons behind the suboptimal treatment of patients with NSTEMI, and recommend approaches to address this issue in order to improve the standard of healthcare for this group of patients. The challenges for the treatment of patients with NSTEMI can be categorized into four "P" factors that contribute to poor clinical outcomes: patient characteristics being heterogeneous; physicians underestimating the high ischemic risk compared with bleeding risk; procedure availability; and policy within the healthcare system. To address these challenges, potential approaches include: developing guidelines and protocols that incorporate rigorous definitions of NSTEMI; risk assessment and integrated quality assessment measures; providing education to physicians on the management of long-term cardiovascular risk in patients with NSTEMI; and making stents and antiplatelet therapies more accessible to patients.
Keywords: antiplatelet therapy; early invasive strategy; non-ST-segment elevation myocardial infarction; treatment-risk paradox.
© 2019 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Figures
References
-
- Jortveit J, Govatsmark RE, Digre TA, et al. Myocardial infarction in Norway in 2013. Tidsskr Nor Laegeforen. 2014;134:1841‐1846. - PubMed
-
- Barrabes JA, Bardaji A, Jimenez‐Candil J, et al. Prognosis and management of acute coronary syndrome in Spain in 2012: the DIOCLES study. Rev Esp Cardiol (Engl Ed). 2015;68:98‐106. - PubMed
-
- Bainey KR, Kaul P, Armstrong PW, et al. Hospital variation in treatment and outcomes in acute coronary syndromes: insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int J Cardiol. 2017;241:70‐75. - PubMed
-
- Chan MY, Sun JL, Newby LK, et al. Long‐term mortality of patients undergoing cardiac catheterization for ST‐elevation and non‐ST‐elevation myocardial infarction. Circulation. 2009;119:3110‐3117. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
