

The profiles of health care utilization among a non-depressed population and patients with depressive symptoms with and without clinical depression
- PMID: 31317810
- PMCID: PMC6713190
- DOI: 10.1080/02813432.2019.1639904
The profiles of health care utilization among a non-depressed population and patients with depressive symptoms with and without clinical depression
Abstract
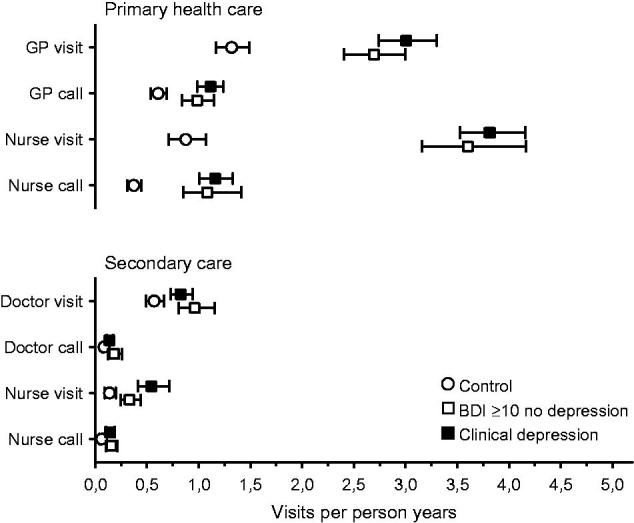
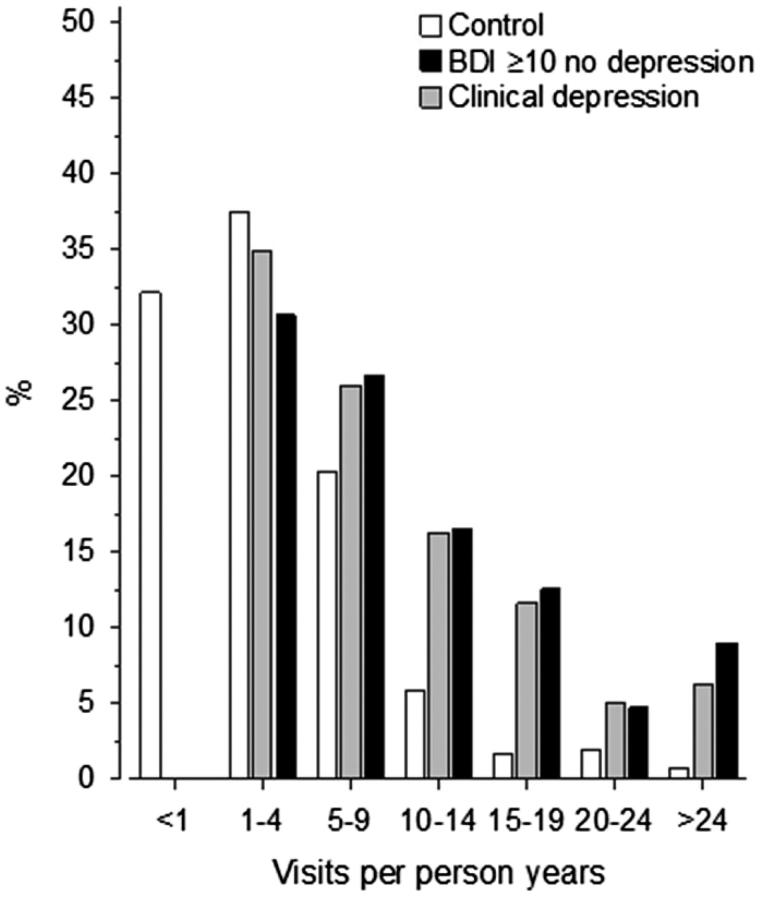
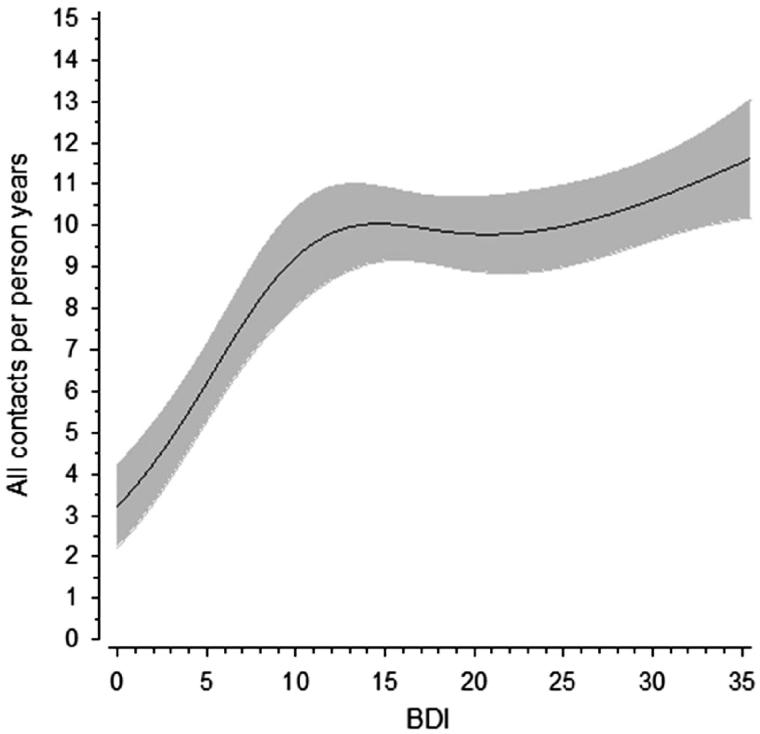
Objective: To examine health service (HS) utilization profiles among a non-depressive population and patients with depressive symptoms (DS) with and without clinical depression. Design, subjects and setting: The study population was based on primary care patients with DS scoring ≥10 in the 21-item Beck Depression Inventory (BDI) and who were at least 35 years old and had been referred to depression nurse case managers (n = 705). Their psychiatric diagnosis was confirmed with the Mini-International Neuropsychiatric Interview (M.I.N.I.). Of these patients, 447 had clinical depression. The number of patients with DS without clinical depression was 258. The control group consisted of a random sample of 414 residents with a BDI score < 10. Use of HS (visits and phone calls to a doctor and a nurse) was based on patient records. Main outcome measures: Number of visits and calls to physicians and nurses. Results: Patients with DS regardless of their depression diagnosis used primary health care (PHC) services three times more than the controls (p < 0.001). In the secondary care, the differences were smaller but significant. Of the controls, 70% had 0-4 HS contacts per year whereas a majority of the patients having DS had more than 5 contacts per year. The number of contacts correlated with the BDI from a score of 0 to 10 but not as clearly in the higher scores. Conclusion: Depressive symptoms, both with or without clinical depression, are associated with increased HS use, especially in PHC. This study suggests that even mild depressive symptoms are associated with an increased use of HS. KEY POINTS We analyzed the health service (HS) use among primary health care patients screened for depression and non-depressive population. Screen positive patients without clinical depression used as much HS as those having clinical depression. Regardless of depression diagnosis, screen positive patients visited a GP and nurse three times more often than the control population. In the screen negative control population, milder depressive symptoms were correlated with the use of HS. Primary health care was responsible for most of the HS use among patients having depressive symptoms.
Keywords: Primary health care; depression; depressive symptoms; health services; public health.
Figures
Similar articles
-
Psychiatric diagnosis in primary care patients with increased depressive symptoms.Nord J Psychiatry. 2019 Apr;73(3):195-199. doi: 10.1080/08039488.2019.1584240. Nord J Psychiatry. 2019. PMID: 30929594
-
Prevalence of restless legs symptoms according to depressive symptoms and depression type: a cross-sectional study.Nord J Psychiatry. 2018 Jan;72(1):51-56. doi: 10.1080/08039488.2017.1385849. Epub 2017 Oct 9. Nord J Psychiatry. 2018. PMID: 28990833
-
Help-seeking intentions and subsequent 12-month mental health service use in Chinese primary care patients with depressive symptoms.BMJ Open. 2015 Jan 28;5(1):e006730. doi: 10.1136/bmjopen-2014-006730. BMJ Open. 2015. PMID: 25631313 Free PMC article.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
-
"Female Preponderance" of Depression in Non-clinical Populations: A Meta-Analytic Study.Front Psychol. 2016 Sep 15;7:1398. doi: 10.3389/fpsyg.2016.01398. eCollection 2016. Front Psychol. 2016. PMID: 27695433 Free PMC article. Review.
Cited by
-
Exploring the impact of mental health conditions on vaccine uptake in high-income countries: a systematic review.BMC Psychiatry. 2023 Jan 7;23(1):15. doi: 10.1186/s12888-022-04512-y. BMC Psychiatry. 2023. PMID: 36611145 Free PMC article.
-
Association between post-stroke depressiveness and the utilization of healthcare services three months after the stroke.Sci Rep. 2025 Aug 2;15(1):28281. doi: 10.1038/s41598-025-12875-x. Sci Rep. 2025. PMID: 40753106 Free PMC article.
-
Excess healthcare costs of mental disorders in children, adolescents and young adults in the Basque population registry adjusted for socioeconomic status and sex.Cost Eff Resour Alloc. 2023 Mar 1;21(1):18. doi: 10.1186/s12962-023-00428-w. Cost Eff Resour Alloc. 2023. PMID: 36859271 Free PMC article.
-
Strengthening Primary Healthcare in Kosovo Requires Tailoring Primary, Secondary and Tertiary Prevention Interventions and Consideration of Mental Health.Front Public Health. 2022 Apr 5;10:794309. doi: 10.3389/fpubh.2022.794309. eCollection 2022. Front Public Health. 2022. PMID: 35480592 Free PMC article.
-
Validation of the Good Spirit, Good Life quality-of-life tool for older Aboriginal Australians.Australas J Ageing. 2023 Jun;42(2):302-310. doi: 10.1111/ajag.13128. Epub 2022 Sep 9. Australas J Ageing. 2023. PMID: 36085595 Free PMC article.
References
-
- Vuorilehto M, Melartin T, Isometsa E. Depressive disorders in primary care: recurrent, chronic, and co-morbid. Psychol Med. 2005;35:673–682. - PubMed
-
- Salokangas RK, Poutanen O, Stengard E, et al. . Prevalence of depression among patients seen in community health centres and community mental health centres. Acta Psychiatr Scand. 1996;93:427–433. - PubMed
-
- Markkula N, Suvisaari J, Saarni SI, et al. . Prevalence and correlates of major depressive disorder and dysthymia in an eleven-year follow-up–results from the Finnish Health 2011 Survey. J Affect Disord. 2015;173:73–80. - PubMed
-
- Kela Sairauspäivärahojen saajat ja maksetut sairauspäivärahat. Accessed 2018 April 27. Available from: http://raportit.kela.fi/ibi_apps/WFServlet?IBIF_ex=NIT098AL.
-
- Global Burden of Disease Study 2013 Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;386:743–800. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical