

Comparison of Biomarker Modalities for Predicting Response to PD-1/PD-L1 Checkpoint Blockade: A Systematic Review and Meta-analysis
- PMID: 31318407
- PMCID: PMC6646995
- DOI: 10.1001/jamaoncol.2019.1549
Comparison of Biomarker Modalities for Predicting Response to PD-1/PD-L1 Checkpoint Blockade: A Systematic Review and Meta-analysis
Abstract
Importance: PD-L1 (programmed cell death ligand 1) immunohistochemistry (IHC), tumor mutational burden (TMB), gene expression profiling (GEP), and multiplex immunohistochemistry/immunofluorescence (mIHC/IF) assays have been used to assess pretreatment tumor tissue to predict response to anti-PD-1/PD-L1 therapies. However, the relative diagnostic performance of these modalities has yet to be established.
Objective: To compare studies that assessed the diagnostic accuracy of PD-L1 IHC, TMB, GEP, and mIHC/IF in predicting response to anti-PD-1/PD-L1 therapy.
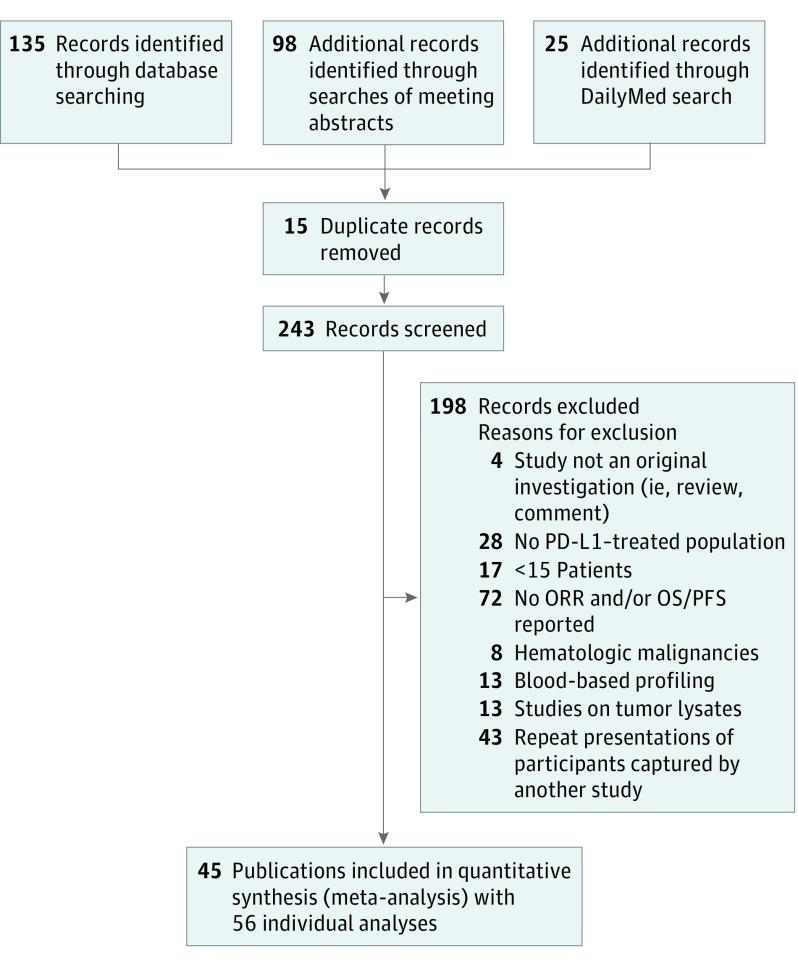
Evidence review: A search of PubMed (from inception to June 2018) and 2013 to 2018 annual meeting abstracts from the American Association for Cancer Research, American Society of Clinical Oncology, European Society for Medical Oncology, and Society for Immunotherapy of Cancer was conducted to identify studies that examined the use of PD-L1 IHC, TMB, GEP, and mIHC/IF assays to determine objective response to anti-PD-1/PD-L1 therapy. For PD-L1 IHC, only clinical trials that resulted in US Food and Drug Administration approval of indications for anti-PD-1/PD-L1 were included. Studies combining more than 1 modality were also included. Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines were followed. Two reviewers independently extracted the clinical outcomes and test results for each individual study.
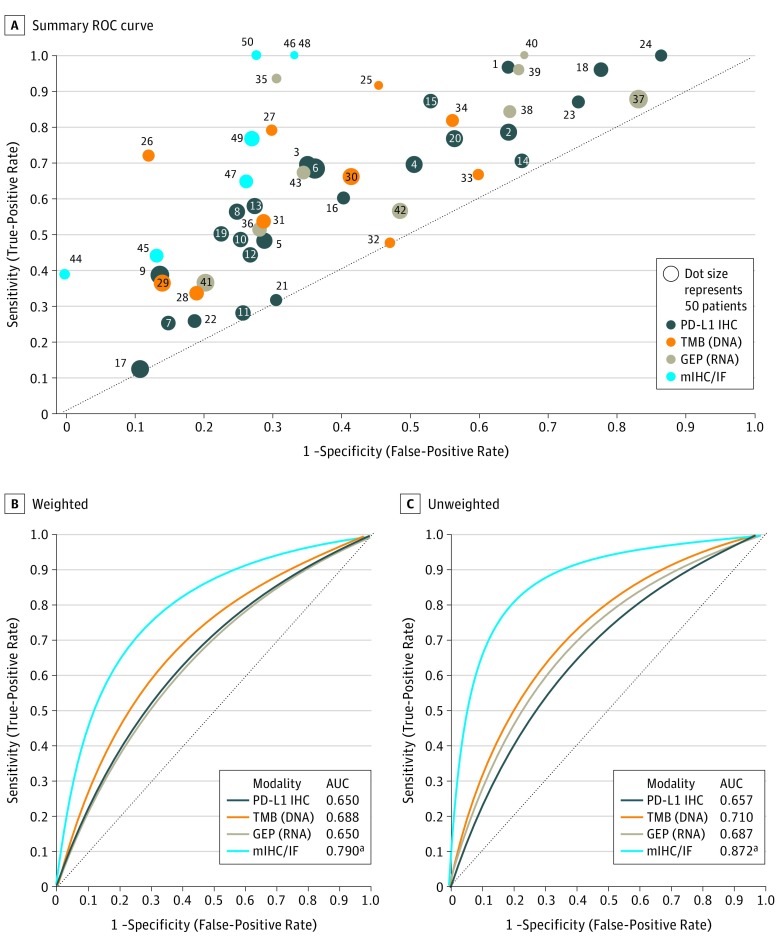
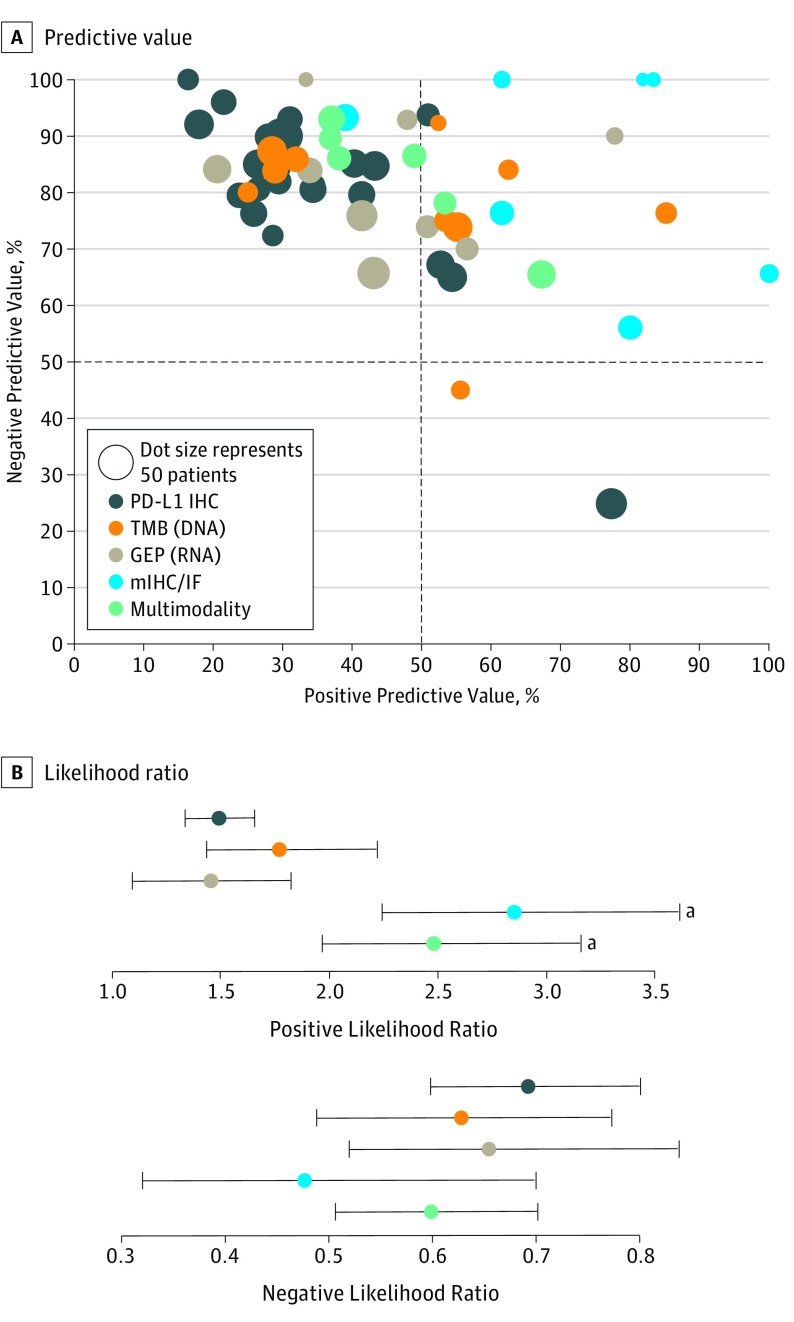
Main outcomes and measures: Summary receiver operating characteristic (sROC) curves; their associated area under the curve (AUC); and pooled sensitivity, specificity, positive and negative predictive values (PPV, NPV), and positive and negative likelihood ratios (LR+ and LR-) for each assay modality.
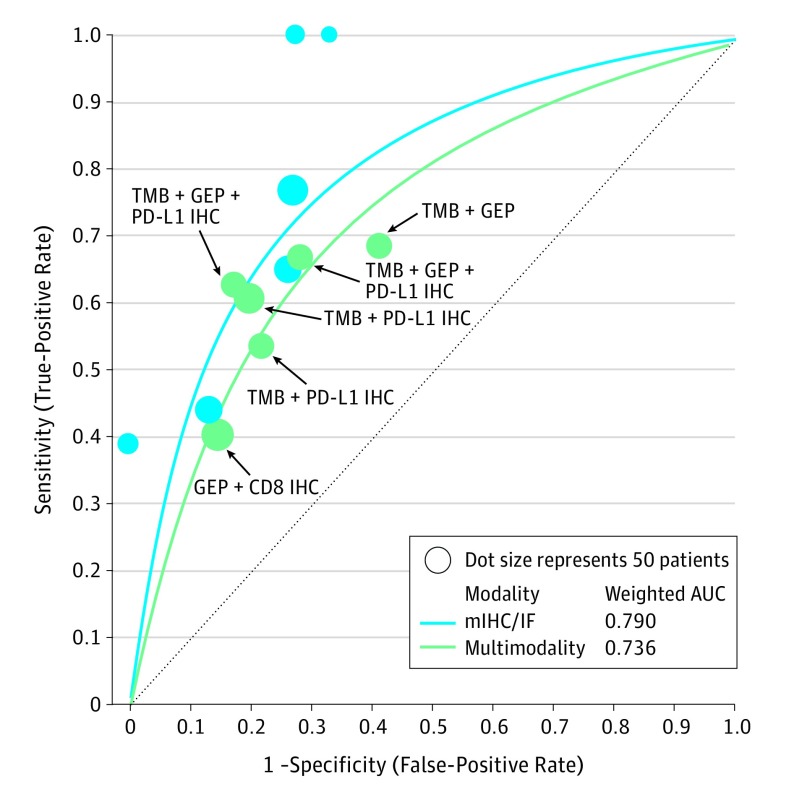
Results: Tumor specimens representing over 10 different solid tumor types in 8135 patients were assayed, and the results were correlated with anti-PD-1/PD-L1 response. When each modality was evaluated with sROC curves, mIHC/IF had a significantly higher AUC (0.79) compared with PD-L1 IHC (AUC, 0.65, P < .001), GEP (AUC, 0.65, P = .003), and TMB (AUC, 0.69, P = .049). When multiple different modalities were combined such as PD-L1 IHC and/or GEP + TMB, the AUC drew nearer to that of mIHC/IF (0.74). All modalities demonstrated comparable NPV and LR-, whereas mIHC/IF demonstrated higher PPV (0.63) and LR+ (2.86) than the other approaches.
Conclusions and relevance: In this meta-analysis, tumor mutational burden, PD-L1 IHC, and GEP demonstrated comparable AUCs in predicting response to anti-PD-1/PD-L1 treatment. Multiplex immunohistochemistry/IF and multimodality biomarker strategies appear to be associated with improved performance over PD-L1 IHC, TMB, or GEP alone. Further studies with mIHC/IF and composite approaches with a larger number of patients will be required to confirm these findings. Additional study is also required to determine the most predictive analyte combinations and to determine whether biomarker modality performance varies by tumor type.
Conflict of interest statement
Figures
Comment in
-
Different Biomarker Modalities and Response to Anti-PD-1/PD-L1 Therapies.JAMA Oncol. 2020 Feb 1;6(2):298-299. doi: 10.1001/jamaoncol.2019.5148. JAMA Oncol. 2020. PMID: 31774455 No abstract available.
-
Different Biomarker Modalities and Response to Anti-PD-1/PD-L1 Therapies-Reply.JAMA Oncol. 2020 Feb 1;6(2):299. doi: 10.1001/jamaoncol.2019.5154. JAMA Oncol. 2020. PMID: 31774476 No abstract available.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
