

Early treated HIV-infected children remain at risk of growth retardation during the first five years of life: Results from the ANRS-PEDIACAM cohort in Cameroon
- PMID: 31318938
- PMCID: PMC6638950
- DOI: 10.1371/journal.pone.0219960
Early treated HIV-infected children remain at risk of growth retardation during the first five years of life: Results from the ANRS-PEDIACAM cohort in Cameroon
Abstract
Background: Long-term growth in HIV-infected infants treated early in resource-limited settings is poorly documented. Incidence of growth retardation, instantaneous risk of death related to malnutrition and growth parameters evolution during the first five years of life of uninfected and early treated HIV-infected children were compared and associated factors with growth retardation were identified.
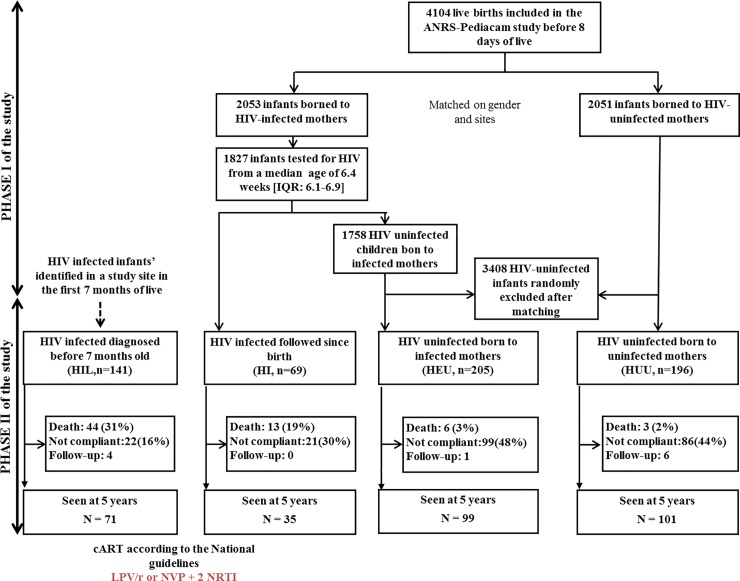
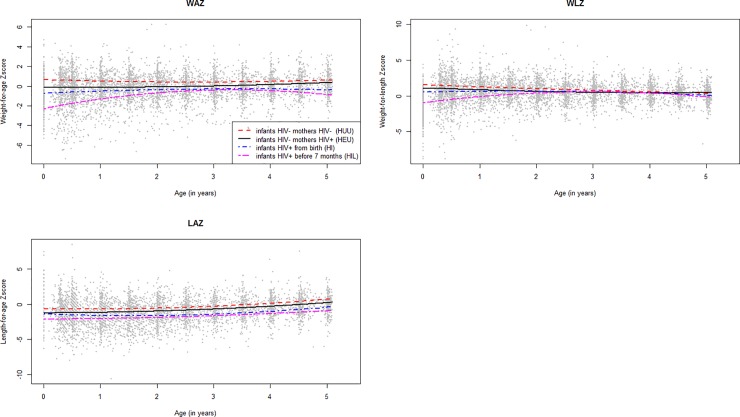
Methods: Weight-for-age (WAZ), weight-for-length (WLZ), and length-for-age (LAZ) Z-scores were calculated. The ANRS-PEDIACAM cohort includes four groups of infants with three enrolled during the first week of life: HIV-infected (HI, n = 69), HIV-exposed uninfected (HEU, n = 205) and HIV-unexposed uninfected (HUU, n = 196). The last group included HIV-infected infants diagnosed before 7 months of age (HIL, n = 141). The multi-state Markov model was used to describe the incidence of growth retardation and identified associated factors.
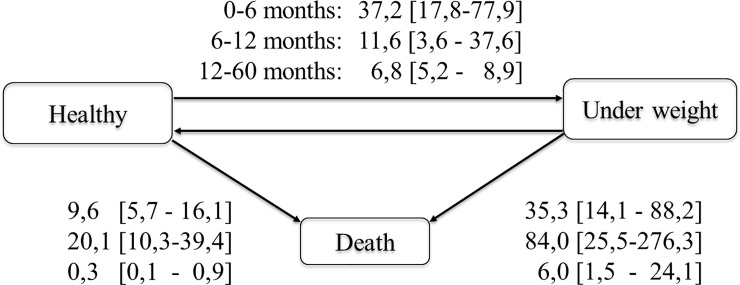
Results: During the first 5 years, 27.5% of children experienced underweight (WAZ<-2), 60.4% stunting (LAZ<-2) and 41.1% wasting (WLZ<-2) at least once. The instantaneous risk of death observed from underweight state (35.3 [14.1-88.2], 84.0 [25.5-276.3], and 6.0 [1.5-24.1] per 1000 person-months for 0-6 months, 6-12 months, and 12-60 months respectively) was higher than from non-underweight state (9.6 [5.7-16.1], 20.1 [10.3-39.4] and 0.3 [0.1-0.9] per 1000 person-months). Compared to HEU, HIL and HI children were most at risk of wasting (adjusted HR (aHR) = 4.3 (95%CI: 1.9-9.8), P<0.001 and aHR = 3.3 (95%CI: 1.4-7.9), P = 0.01 respectively) and stunting for HIL (aHR = 8.4 (95%CI: 2.4-29.7). The risk of underweight was higher in HEU compared to HUU children (aHR = 5.0 (CI: 1.4-10.0), P = 0.001). Others associated factors to growth retardation were chronic pathologies, small size at birth, diarrhea and CD4< 25%.
Conclusions: HIV-infected children remained at high risk of wasting and stunting within the first 5 years period of follow-up. There is a need of identifying suitable nutritional support and best ways to integrate it with cART in pediatric HIV infection global care.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Alimentation du nourrisson et du jeune enfant. Aide-mémoire N° 342Juillet 2015. 02/06/2016. Available from: http://www.who.int/mediacentre/factsheets/fs342/fr/.
-
- UNICEF. Committing to Child Survival: A Promise Renewed. Progress Report 2014. 3 United Nations Plaza, New York, NY 10017, USA: UNICEF; Septembre 2014.
-
- UNAIDS. UNAIDS gap report 2014.2014:[26 p.]. Available from: http://www.unaids.org/fr/resources/campaigns/2014/2014gapreport/gapreport.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
