

Blood pressure and risk of cancer in the European Prospective Investigation into Cancer and Nutrition
- PMID: 31319002
- PMCID: PMC7115826
- DOI: 10.1002/ijc.32576
Blood pressure and risk of cancer in the European Prospective Investigation into Cancer and Nutrition
Abstract
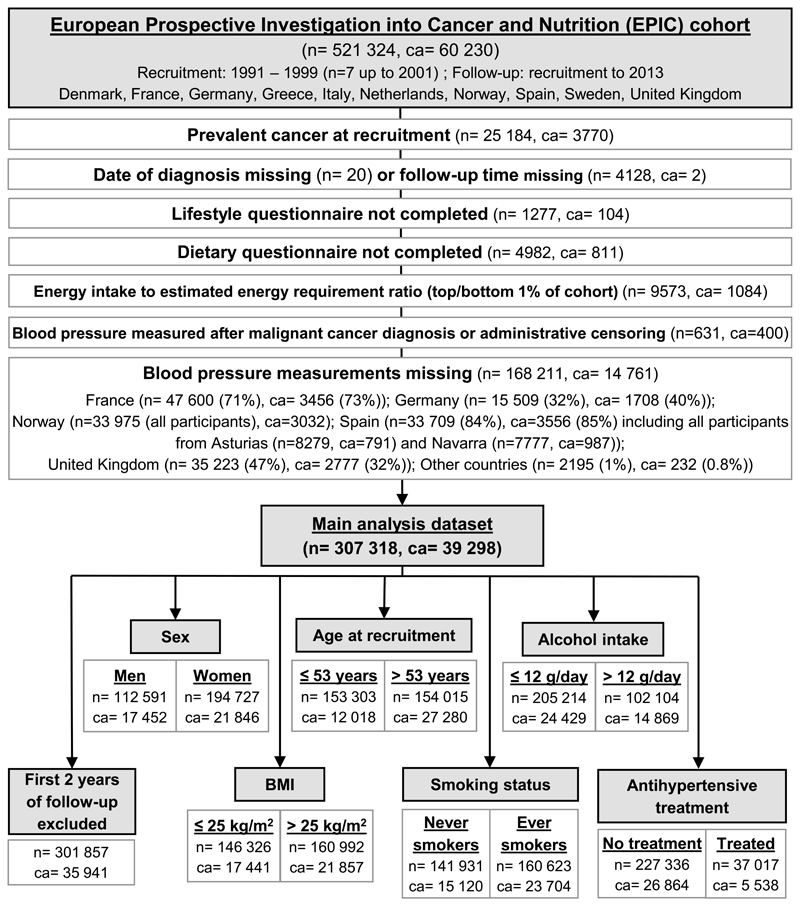
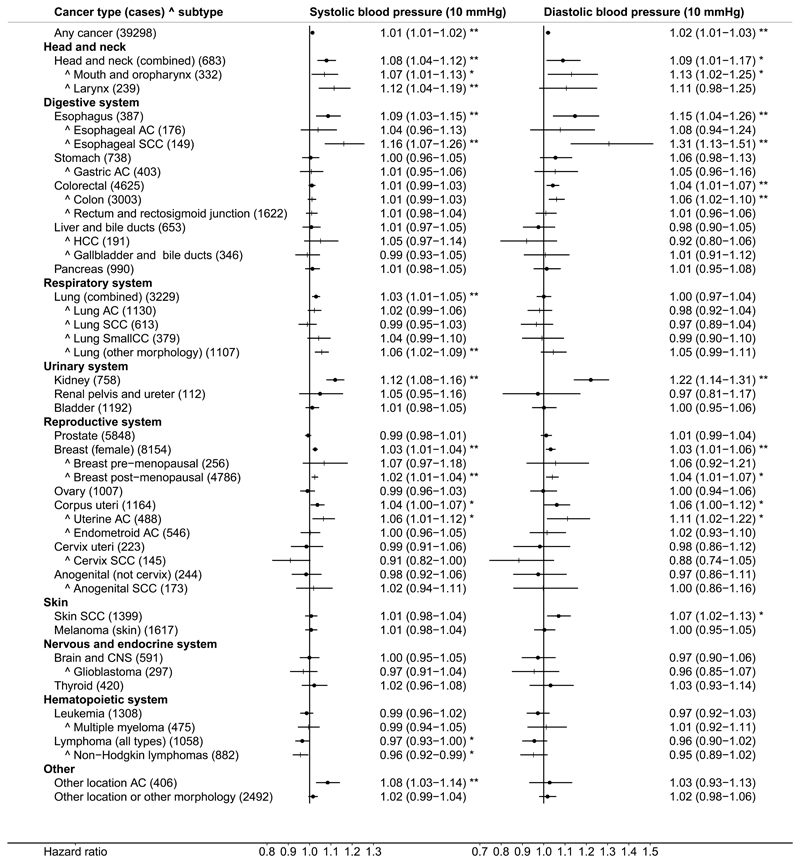
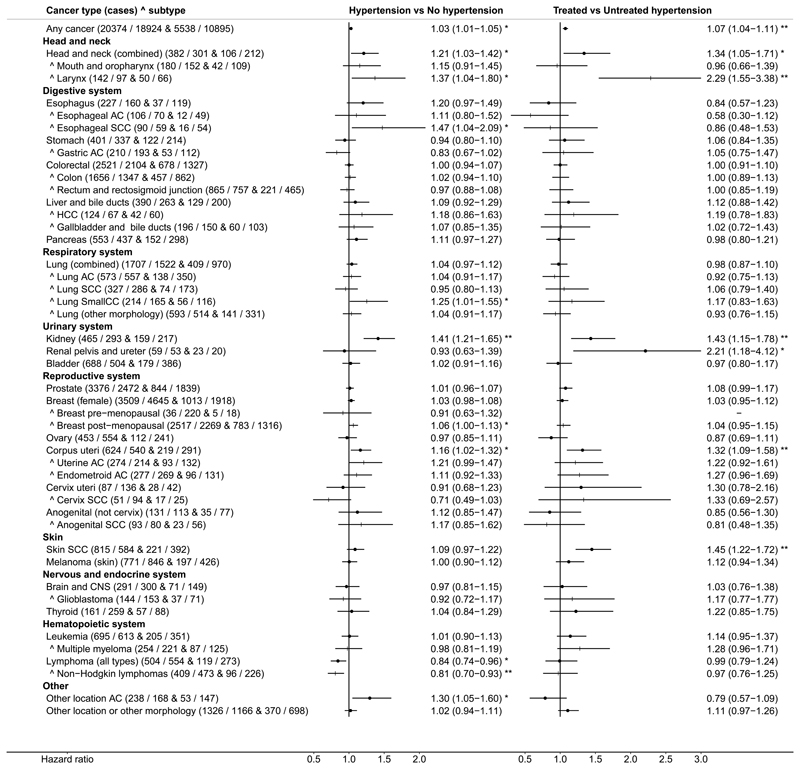
Several studies have reported associations of hypertension with cancer, but not all results were conclusive. We examined the association of systolic (SBP) and diastolic (DBP) blood pressure with the development of incident cancer at all anatomical sites in the European Prospective Investigation into Cancer and Nutrition (EPIC). Hazard ratios (HRs) (95% confidence intervals) were estimated using multivariable Cox proportional hazards models, stratified by EPIC-participating center and age at recruitment, and adjusted for sex, education, smoking, body mass index, physical activity, diabetes and dietary (in women also reproductive) factors. The study included 307,318 men and women, with an average follow-up of 13.7 (standard deviation 4.4) years and 39,298 incident cancers. We confirmed the expected positive association with renal cell carcinoma: HR = 1.12 (1.08-1.17) per 10 mm Hg higher SBP and HR = 1.23 (1.14-1.32) for DBP. We additionally found positive associations for esophageal squamous cell carcinoma (SCC): HR = 1.16 (1.07-1.26) (SBP), HR = 1.31 (1.13-1.51) (DBP), weaker for head and neck cancers: HR = 1.08 (1.04-1.12) (SBP), HR = 1.09 (1.01-1.17) (DBP) and, similarly, for skin SCC, colon cancer, postmenopausal breast cancer and uterine adenocarcinoma (AC), but not for esophageal AC, lung SCC, lung AC or uterine endometroid cancer. We observed weak inverse associations of SBP with cervical SCC: HR = 0.91 (0.82-1.00) and lymphomas: HR = 0.97 (0.93-1.00). There were no consistent associations with cancers in other locations. Our results are largely compatible with published studies and support weak associations of blood pressure with cancers in specific locations and morphologies.
Keywords: Europe; association; cancer; cohort; epidemiology; hypertension; morphology; risk factors.
© 2019 UICC.
Conflict of interest statement
Figures
References
-
- Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392:1923–1994. - PMC - PubMed
-
- Zhou B, Bentham J, Di Cesare M, Bixby H, Danaei G, Cowan MJ, Paciorek CJ, Singh G, Hajifathalian K, Bennett JE, Taddei C, et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. The Lancet. 2017;389:37–55. - PMC - PubMed
-
- Stocks T, Van Hemelrijck M, Manjer J, Bjorge T, Ulmer H, Hallmans G, Lindkvist B, Selmer R, Nagel G, Tretli S, Concin H, et al. Blood pressure and risk of cancer incidence and mortality in the Metabolic Syndrome and Cancer Project. Hypertension. 2012;59:802–810. - PubMed
-
- Grossman E, Messerli FH, Boyko V, Goldbourt U. Is there an association between hypertension and cancer mortality? Am J Med. 2002;112:479–486. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
