

The Effect of High-Dose Postpartum Maternal Vitamin D Supplementation Alone Compared with Maternal Plus Infant Vitamin D Supplementation in Breastfeeding Infants in a High-Risk Population. A Randomized Controlled Trial
- PMID: 31319554
- PMCID: PMC6682993
- DOI: 10.3390/nu11071632
The Effect of High-Dose Postpartum Maternal Vitamin D Supplementation Alone Compared with Maternal Plus Infant Vitamin D Supplementation in Breastfeeding Infants in a High-Risk Population. A Randomized Controlled Trial
Abstract
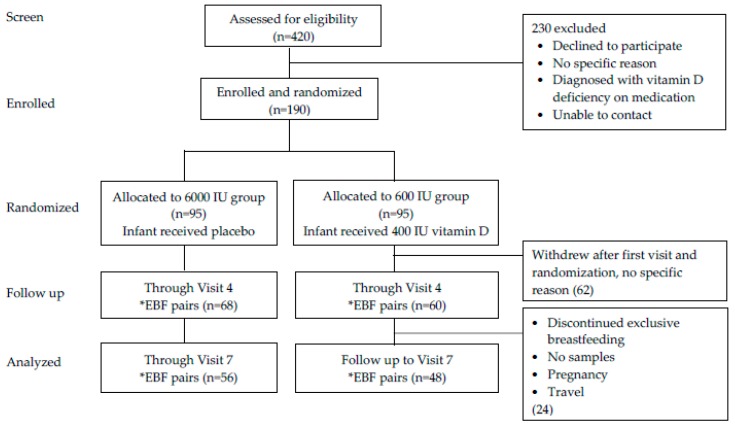
In view of continuing reports of high prevalence of severe vitamin D deficiency and low rate of infant vitamin D supplementation, an alternative strategy for prevention of vitamin D deficiency in infants warrants further study. The aim of this randomized controlled trial among 95 exclusively breastfeeding mother-infant pairs with high prevalence of vitamin D deficiency was to compare the effect of six-month post-partum vitamin D3 maternal supplementation of 6000 IU/day alone with maternal supplementation of 600 IU/day plus infant supplementation of 400 IU/day on the vitamin D status of breastfeeding infants in Doha, Qatar. Serum calcium, parathyroid hormone, maternal urine calcium/creatinine ratio and breast milk vitamin D content were measured. At baseline, the mean serum 25-hydroxyvitamin D (25(OH)D) of mothers on 6000 IU and 600 IU (35.1 vs. 35.7 nmol/L) and in their infants (31.9 vs. 29.6) respectively were low but similar. At the end of the six month supplementation, mothers on 6000 IU achieved higher serum 25(OH)D mean ± SD of 98 ± 35 nmol/L than 52 ± 20 nmol/L in mothers on 600 IU (p < 0.0001). Of mothers on 6000 IU, 96% achieved adequate serum 25(OH)D (≥50 nmol/L) compared with 52%in mothers on 600 IU (p < 0.0001). Infants of mothers on 600 IU and also supplemented with 400 IU vitamin D3 had slightly higher serum 25(OH)D than infants of mothers on 6000 IU alone (109 vs. 92 nmol/L, p = 0.03); however, similar percentage of infants in both groups achieved adequate serum 25(OH)D ≥50 nmol/L (91% vs. 89%, p = 0.75). Mothers on 6000 IU vitamin D3/day also had higher human milk vitamin D content. Safety measurements, including serum calcium and urine calcium/creatinine ratios in the mother and serum calcium levels in the infants were similar in both groups. Maternal 6000 IU/day vitamin D3 supplementation alone safely optimizes maternal vitamin D status, improves milk vitamin D to maintain adequate infant serum 25(OH)D. It thus provides an alternative option to prevent the burden of vitamin D deficiency in exclusively breastfeeding infants in high-risk populations and warrants further study of the effective dose.
Keywords: breastfeeding; infants; mothers; supplementation; vitamin D deficiency.
Conflict of interest statement
The authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analysis or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures

References
-
- Munns C.F., Shaw N., Kiely M., Specker B.L., Thacher T.D., Ozono K., Michigami T., Tiosano D., Mughal M.Z., Makitie O., et al. Global consensus recommendations on prevention and management of nutritional rickets. J. Clin. Endocrinol. Metab. 2016;101:394–415. doi: 10.1210/jc.2015-2175. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
