

Overweight/obesity affects histological features and inflammatory gene signature of synovial membrane of Rheumatoid Arthritis
- PMID: 31320744
- PMCID: PMC6639364
- DOI: 10.1038/s41598-019-46927-w
Overweight/obesity affects histological features and inflammatory gene signature of synovial membrane of Rheumatoid Arthritis
Abstract
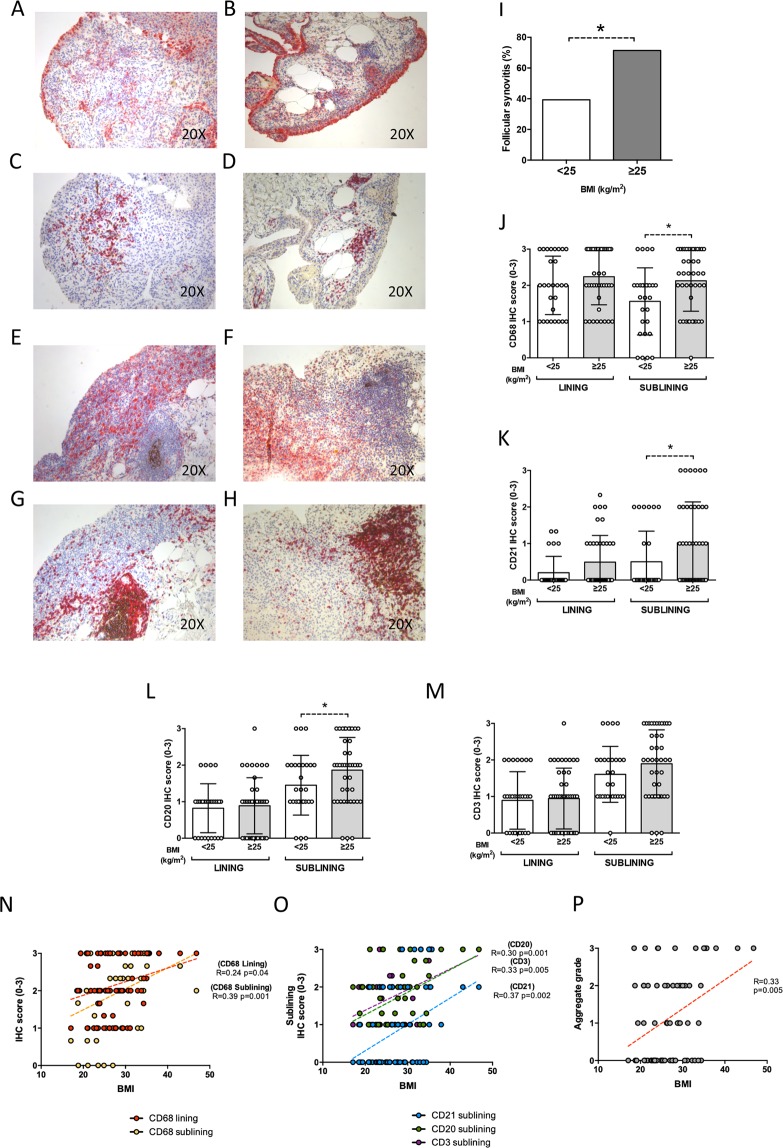
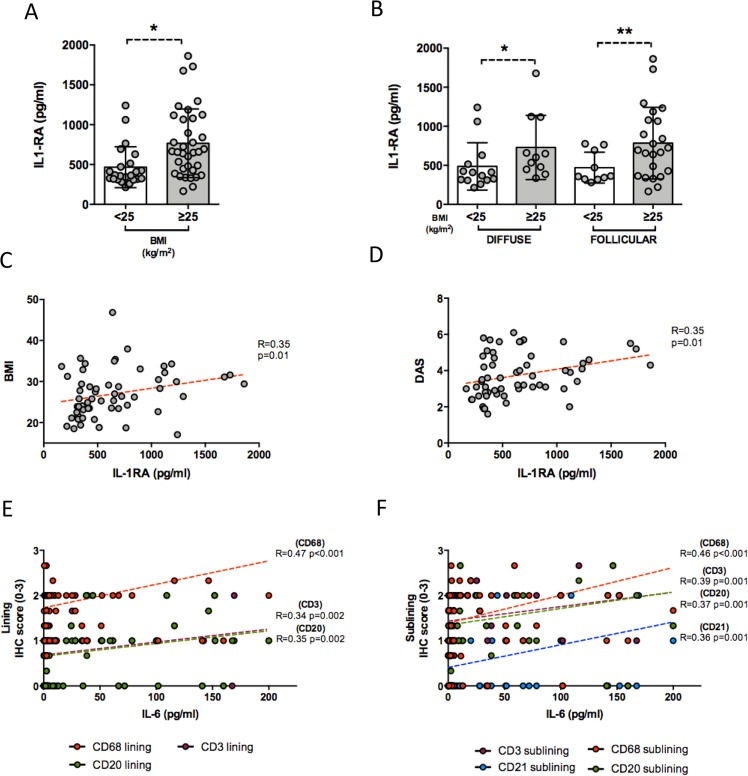
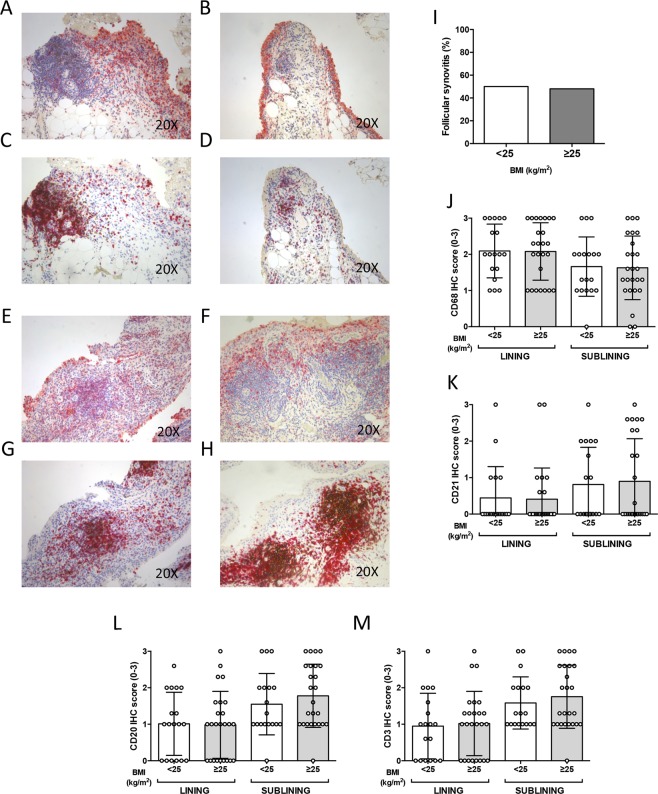
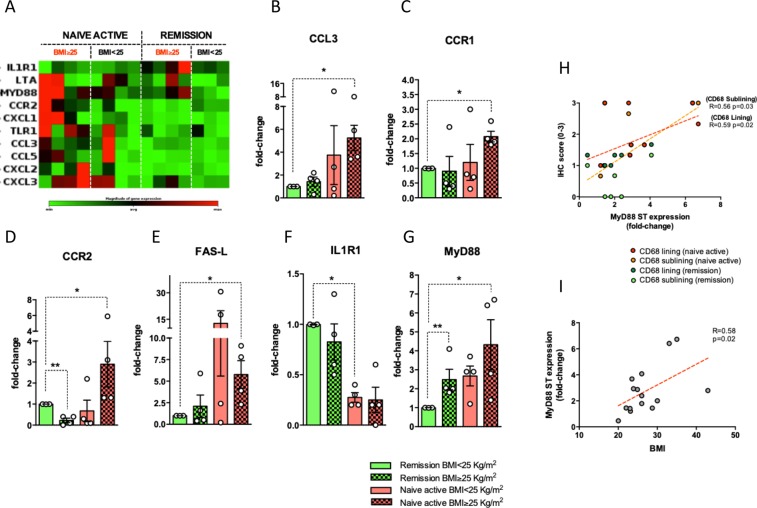
Overweight/obesity influence disease burden and clinical outcome of Rheumatoid Arthritis (RA). The impact of overweight/obesity on synovial tissue (ST) inflammation is largely unknown. Here, we investigated the histological and transcriptional signature of ST obtained from RA in different disease phases (disease onset, failure to first-line conventional DMARDs and in sustained clinical and ultrasound remission) finding that overweight/obese DMARDs naive RA showed higher likelihood of follicular synovitis, higher IHC scores for sublining inflammatory cells (CD68+, CD21+ and CD20+) and higher IL-1RA plasma levels than normal weight RA. Regardless to the synovitis pattern, overweight/obese DMARDs naive RA showed a worse clinical response to "Treat-to-target" (T2T) than normal weight RA at 6 and 12 months follow-up. Conversely, MTX-IR RA did not show significant differences in synovial inflammation based on BMI category. Overweight/obese RA in stable clinical and US remission showed higher degree of residual synovitis in terms of sublining CD68+, CD20+ cells and lining and sublining CD3+ compared to normal weight RA. Finally, gene expression profile analysis revealed that ST of overweight/obese DMARDs naive RA is enriched by CCL3 and MyD88 compared to normal weight RA in sustained disease remission, the latter correlating with BMI and IHC scores for synovial CD68+ cells. These findings suggest that indeed overweight/obese RA show higher degree of synovitis at disease onset and after remission achievement that influences the response rate to T2T and should be considered within the management of patients with RA.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
