

Current Technique for the Ream-and-Run Arthroplasty for Glenohumeral Osteoarthritis
- PMID: 31321140
- PMCID: PMC6554086
- DOI: 10.2106/JBJS.ST.L.00009
Current Technique for the Ream-and-Run Arthroplasty for Glenohumeral Osteoarthritis
Abstract
Introduction: The ream and run is a technically demanding shoulder arthroplasty for the management of glenohumeral arthritis that avoids the risk of failure of the glenoid component that is associated with total shoulder arthroplasty.
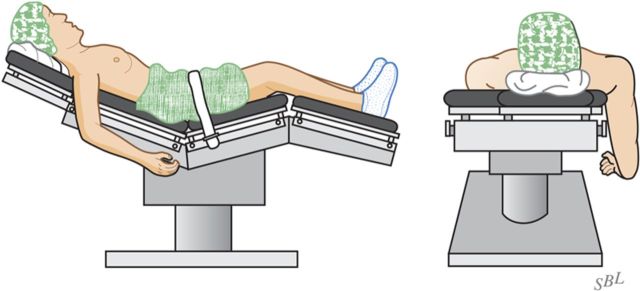
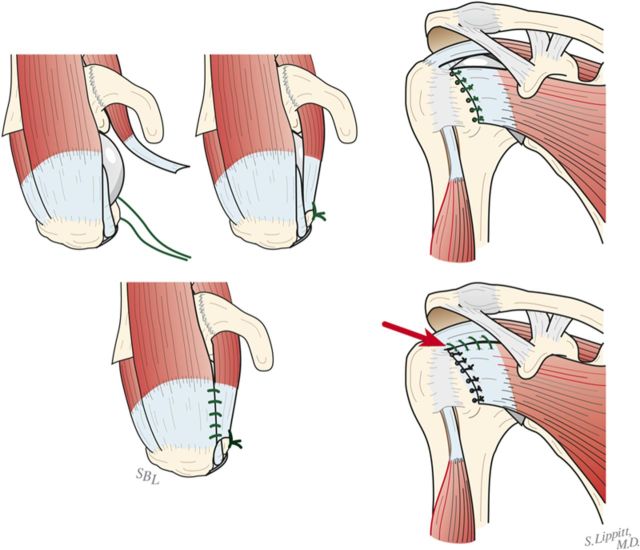
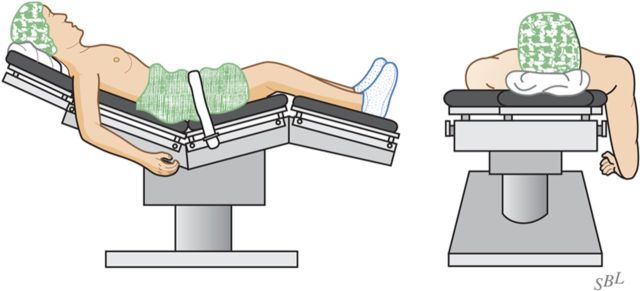
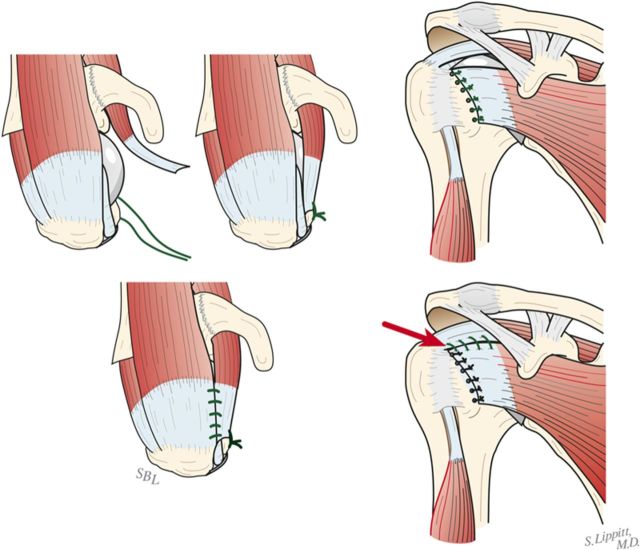
Step 1 surgical approach: After administration of prophylactic antibiotics and a thorough skin preparation, expose the glenohumeral joint through a long deltopectoral incision, incising the subscapularis tendon from its osseous insertion and the capsule from the anterior-inferior aspect of the humeral neck while carefully protecting all muscle groups and neurovascular structures.
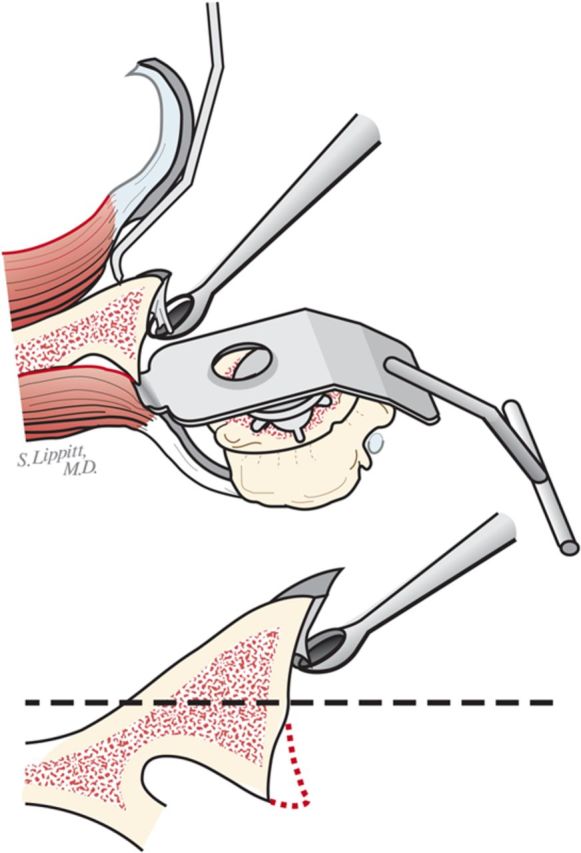
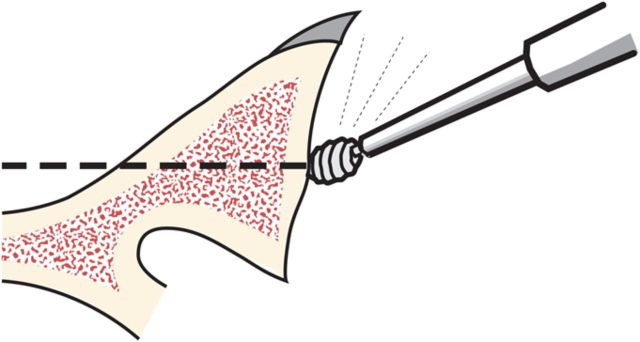
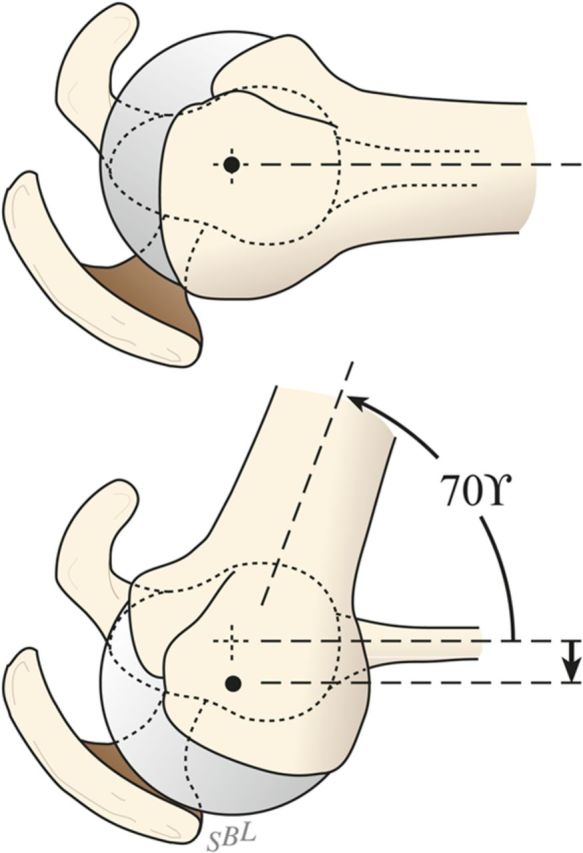
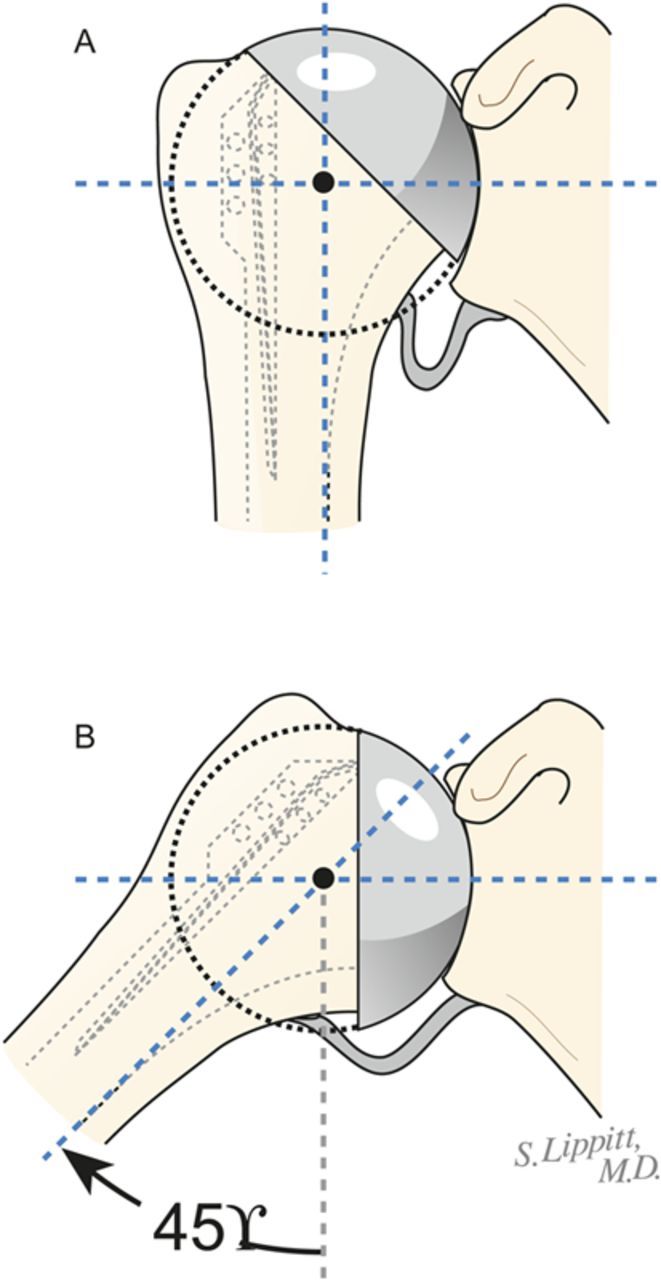
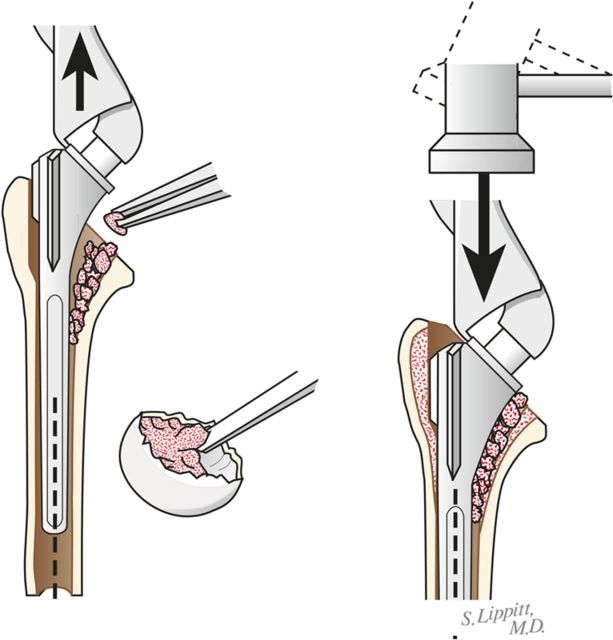
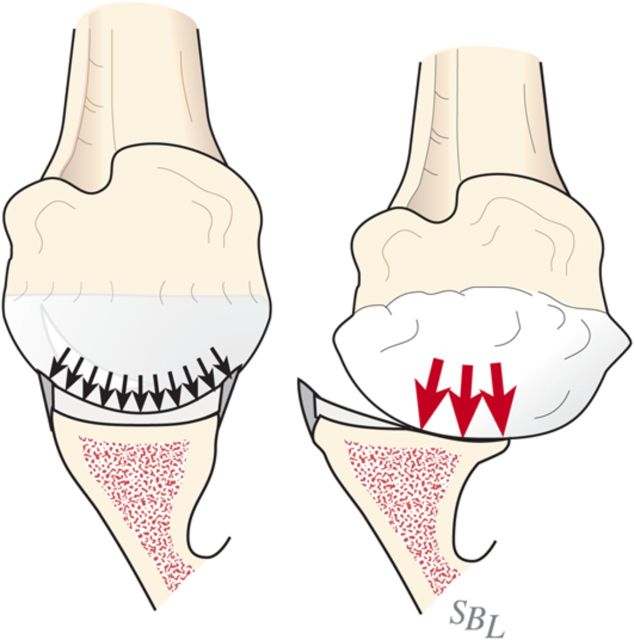
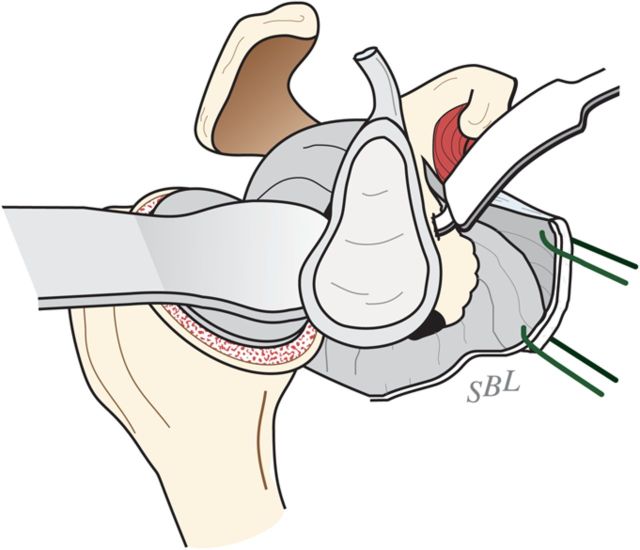
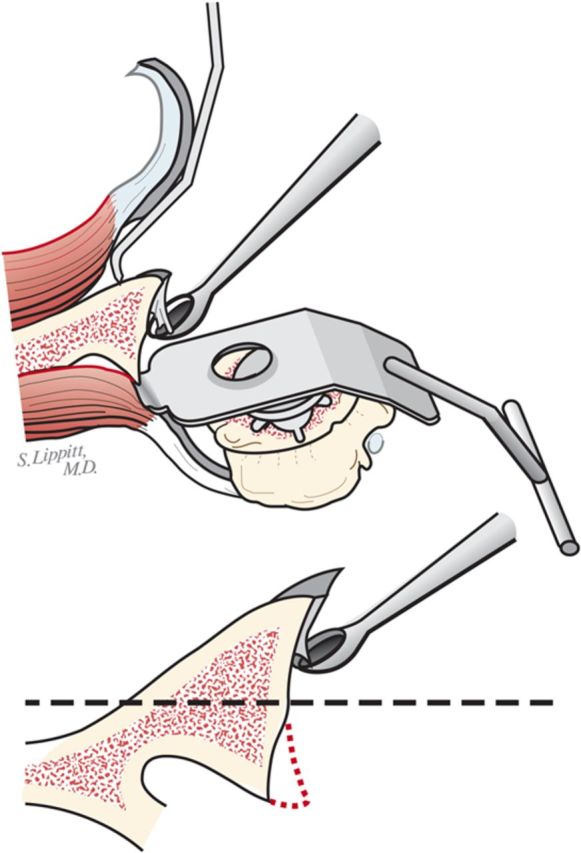
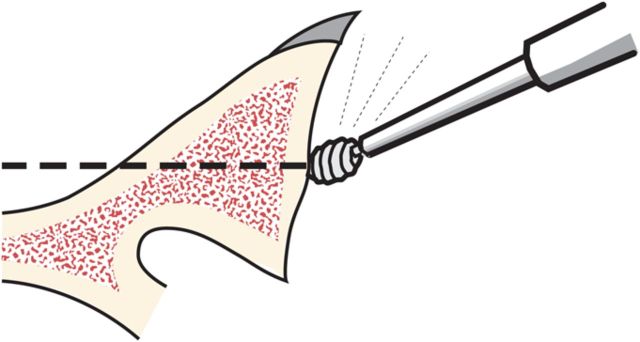
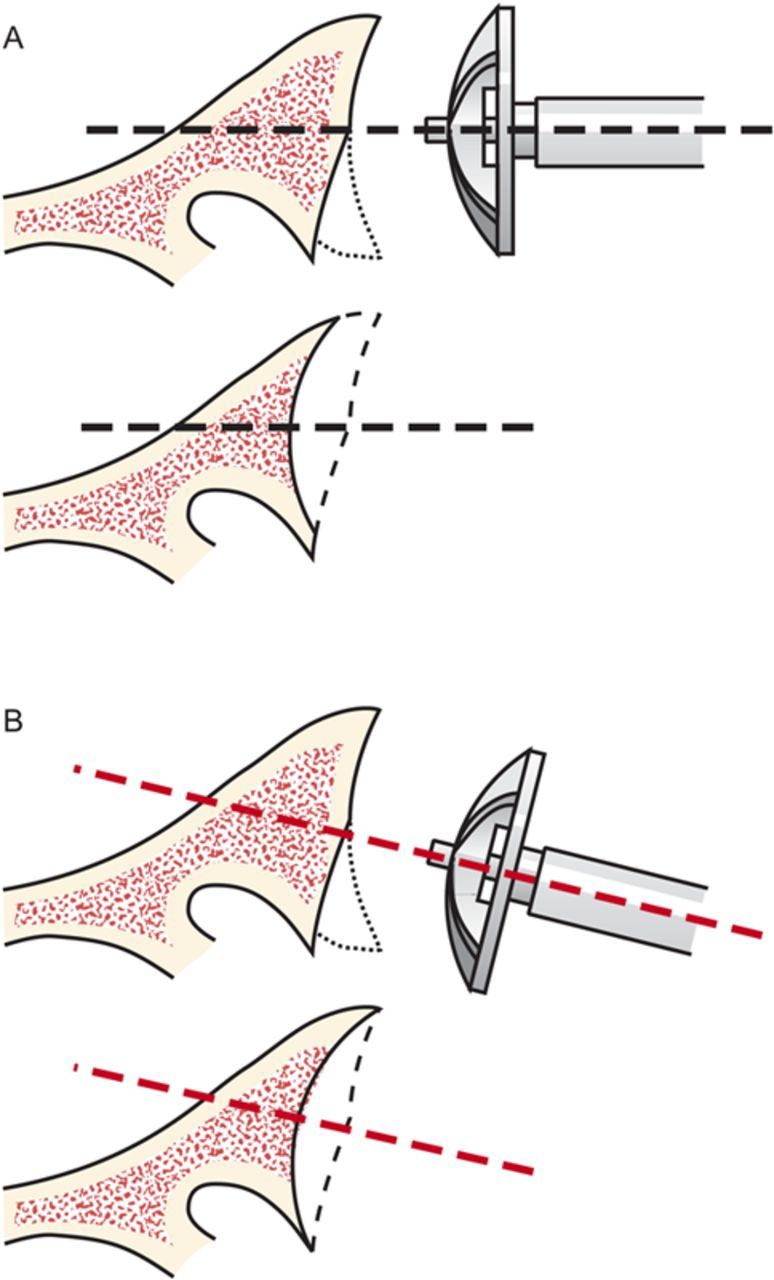
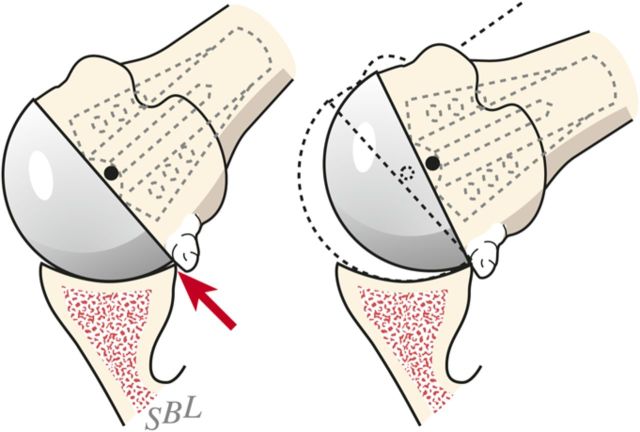
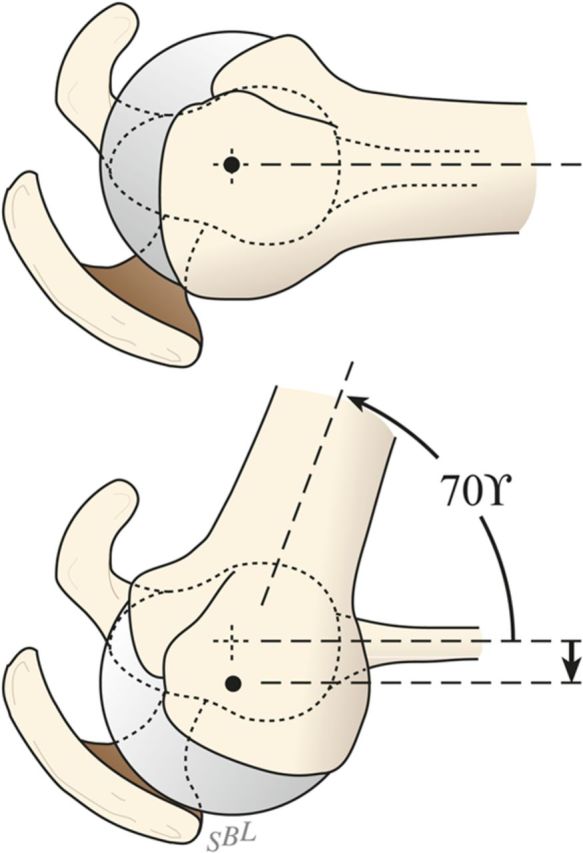
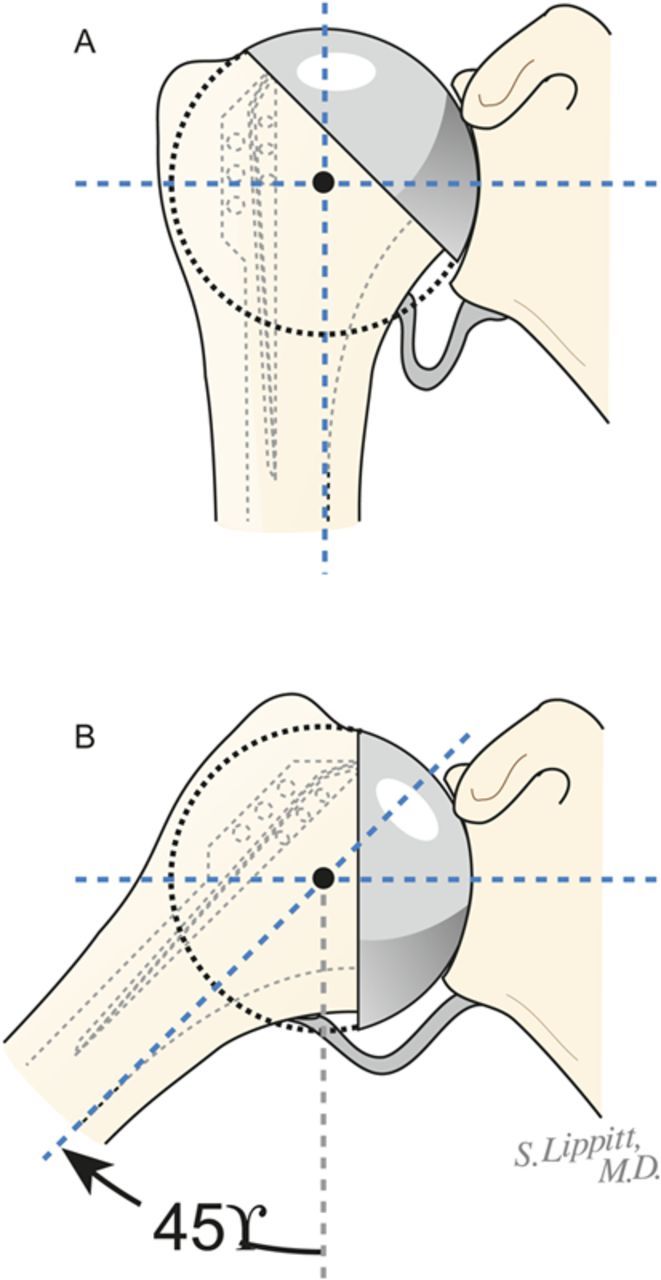
Step 2 humeral preparation: Gently expose the proximal part of the humerus, resect the humeral head at 45° to the orthopaedic axis while protecting the rotator cuff, and excise all humeral osteophytes.
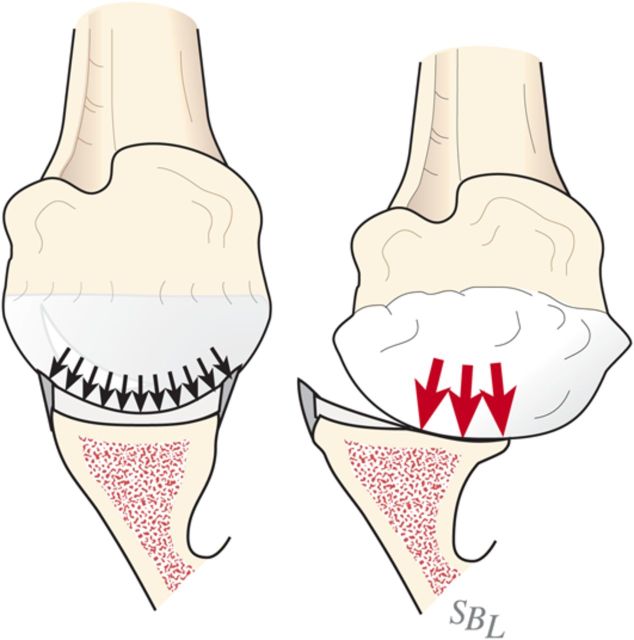
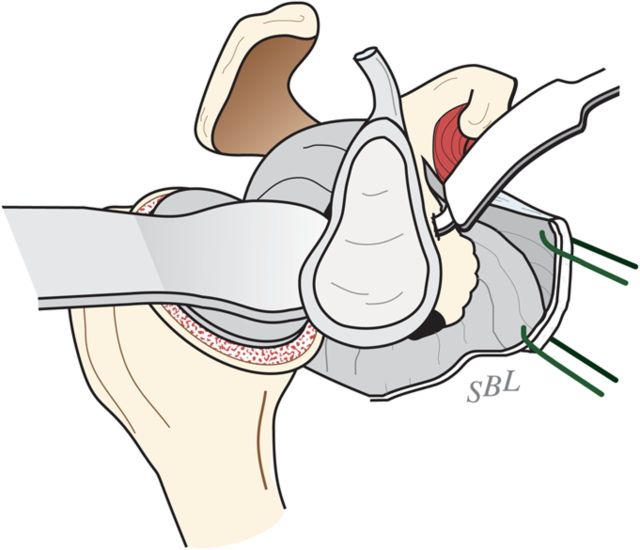
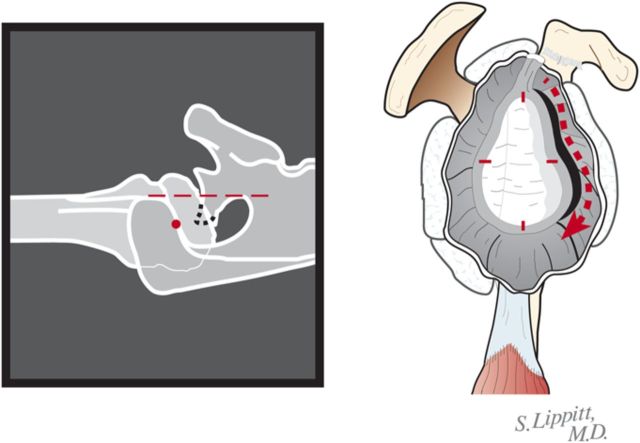
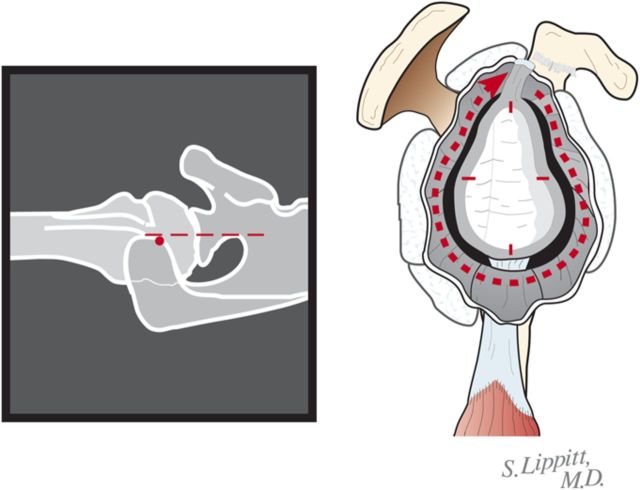
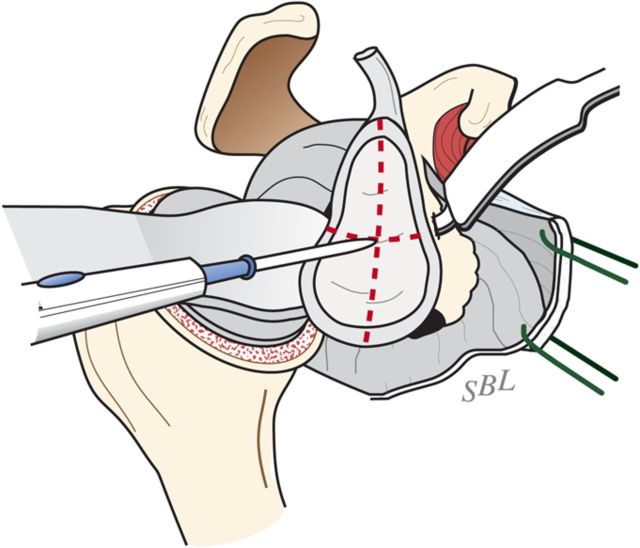
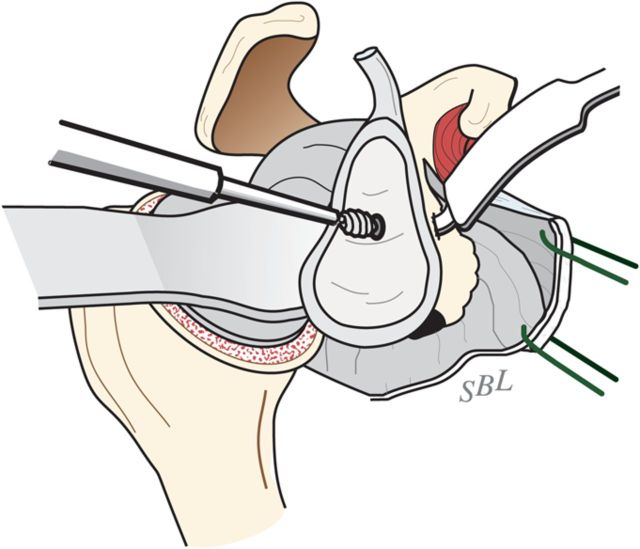
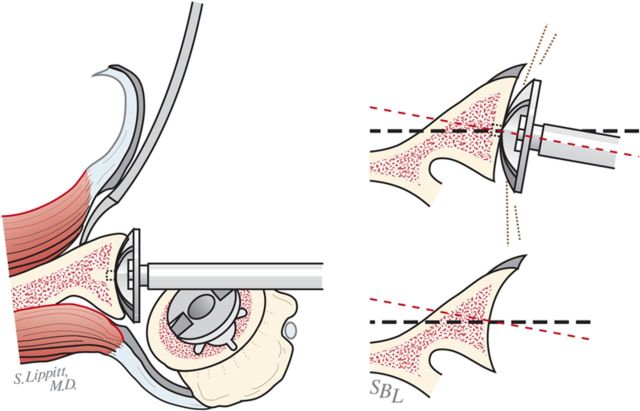
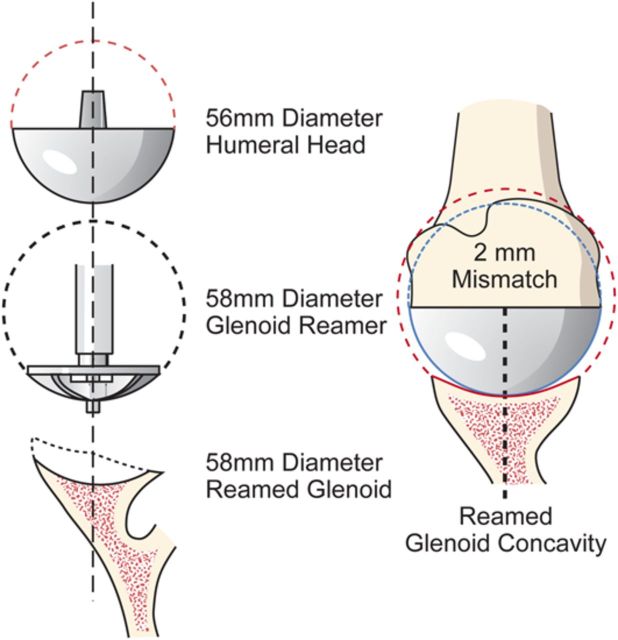
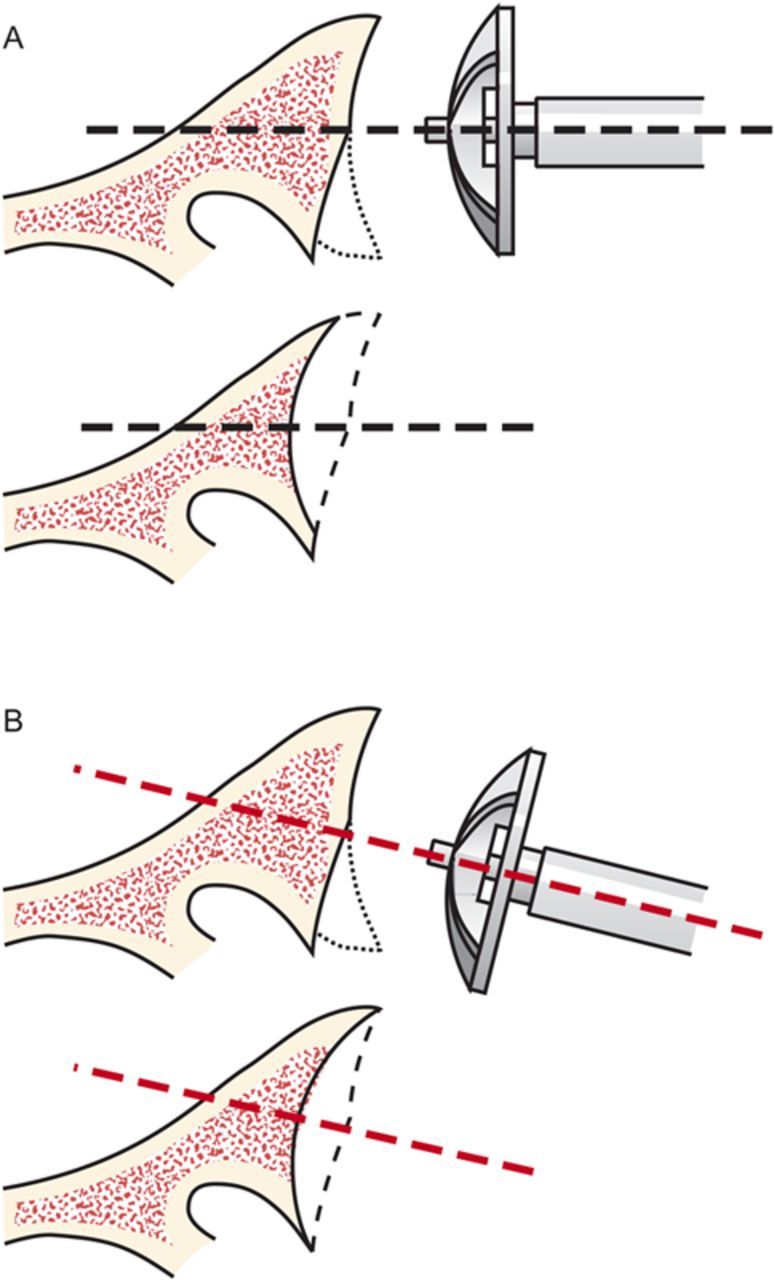
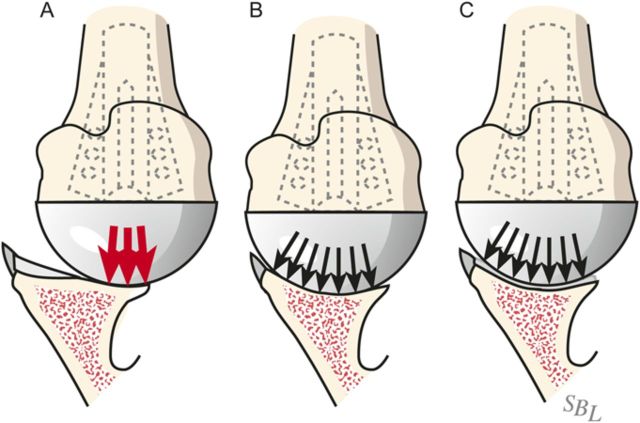
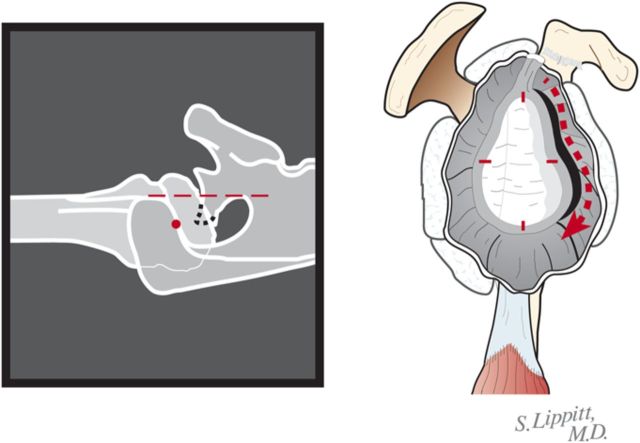
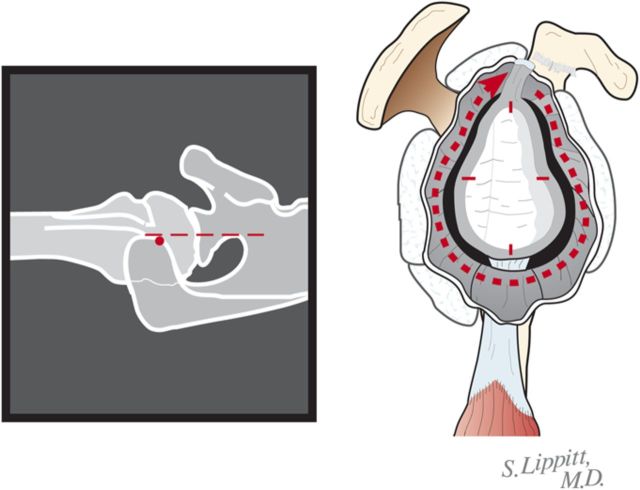
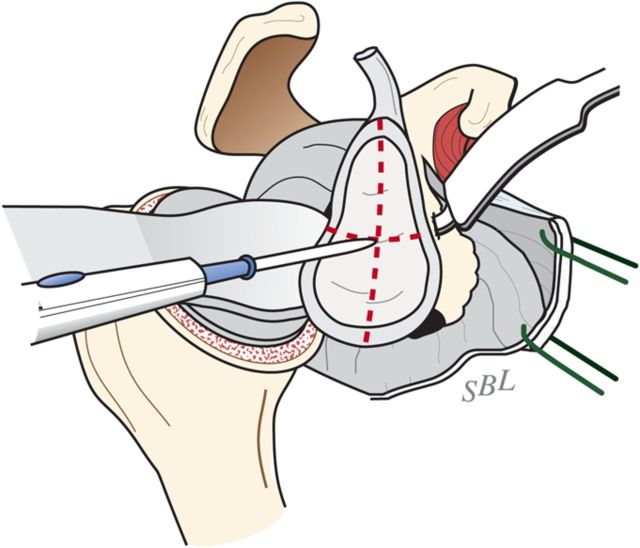
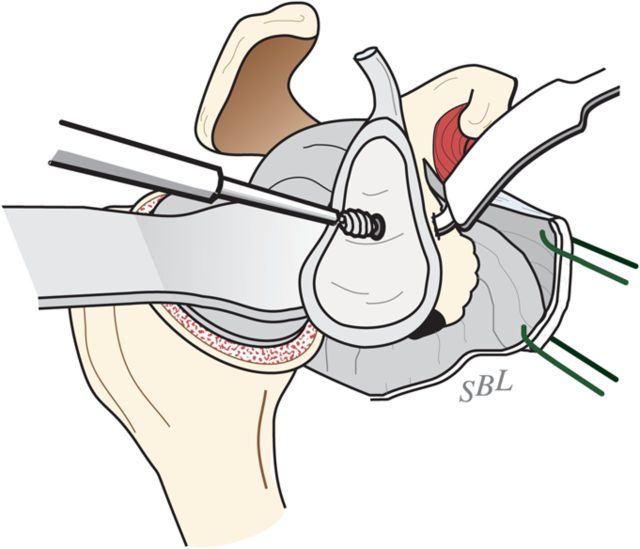
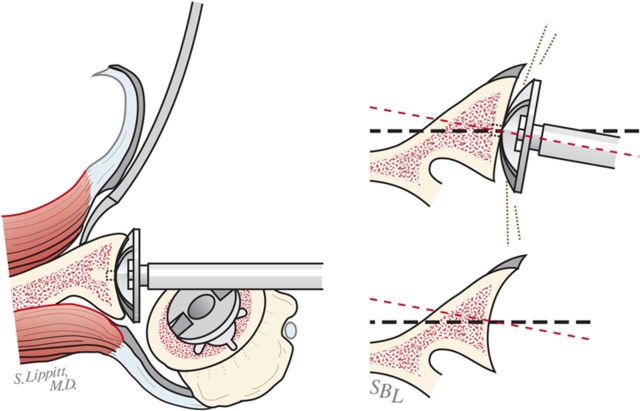
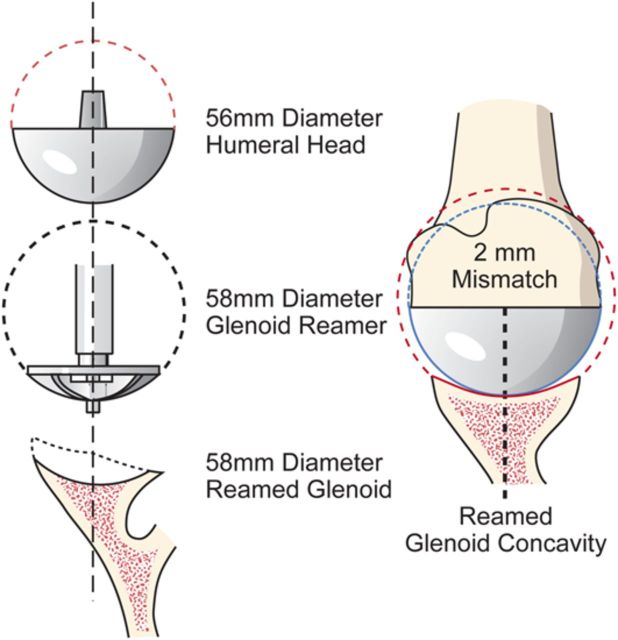
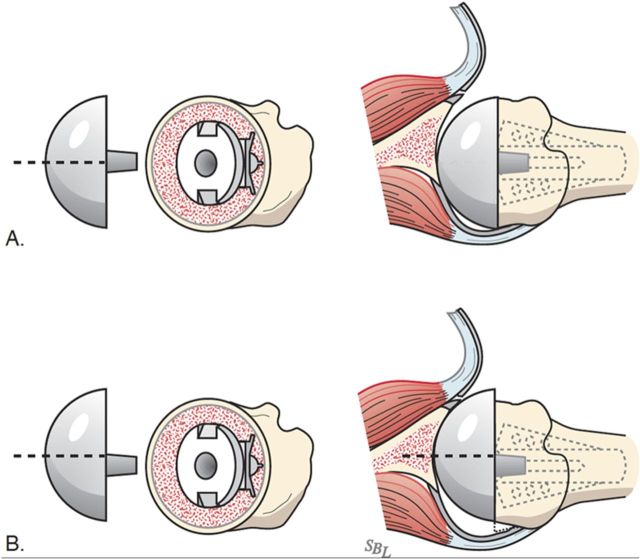
Step 3 glenoid preparation: After performing an extralabral capsular release, remove any residual cartilage, drill the glenoid centerline, and ream the glenoid to a single concavity.
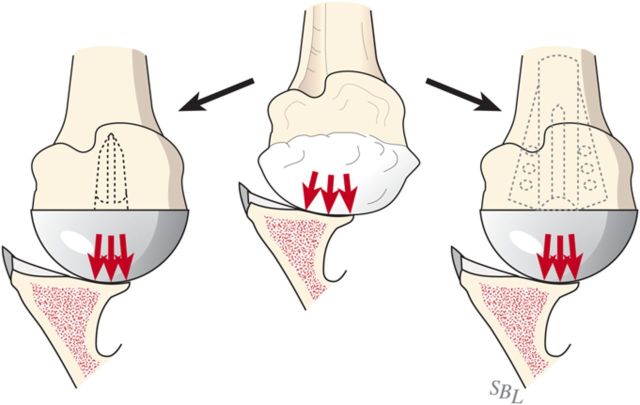
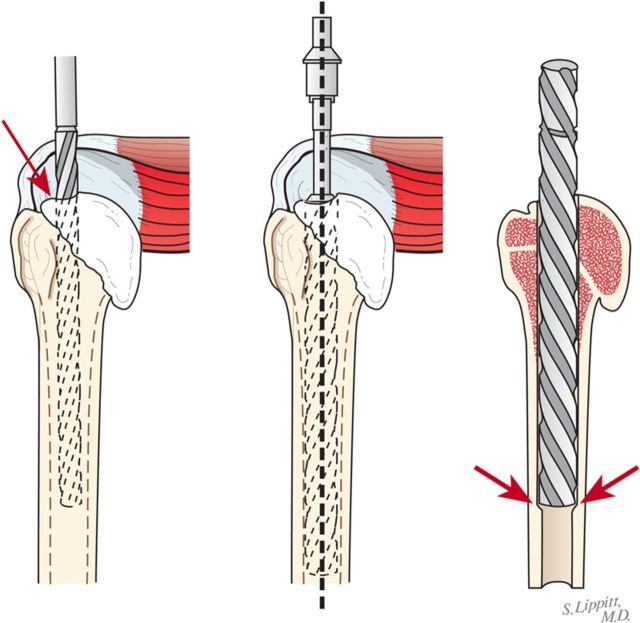
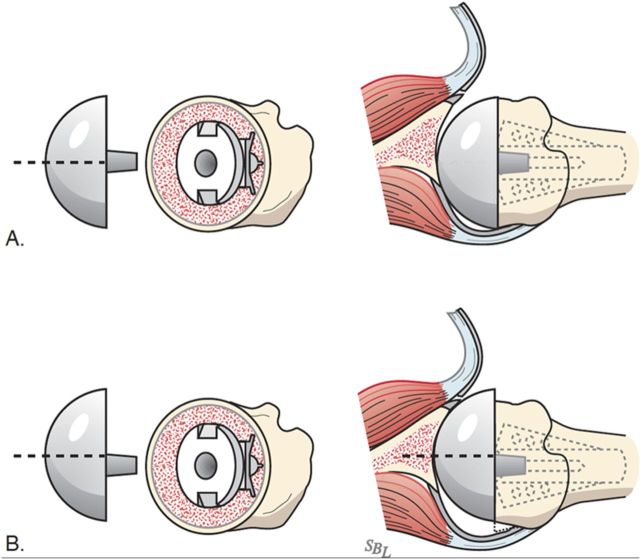
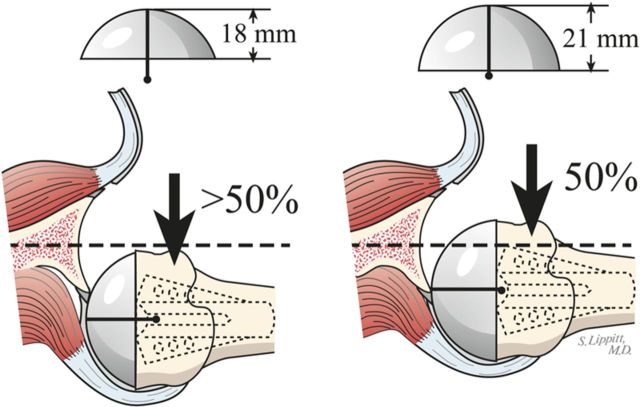
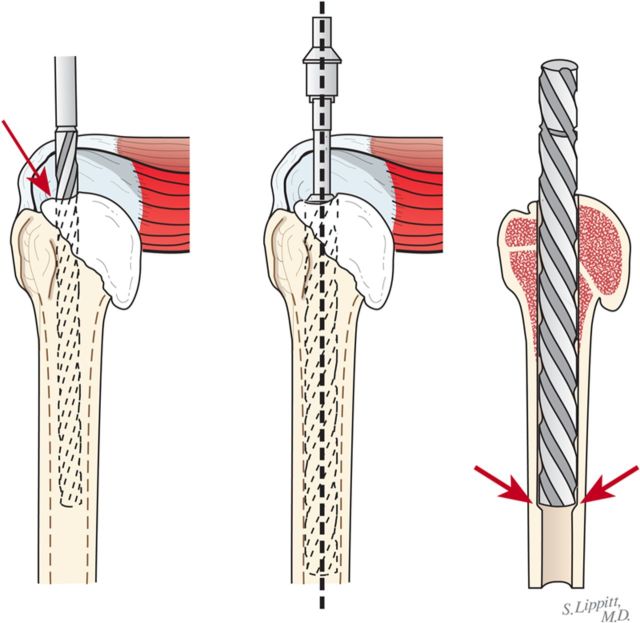
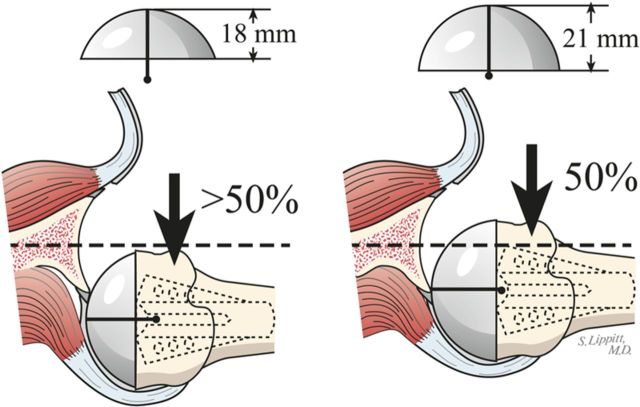
Step 4 humeral prosthesis selection: Select a humeral prosthesis that fits the medullary canal and that provides the desired mobility and stability of the prosthesis.
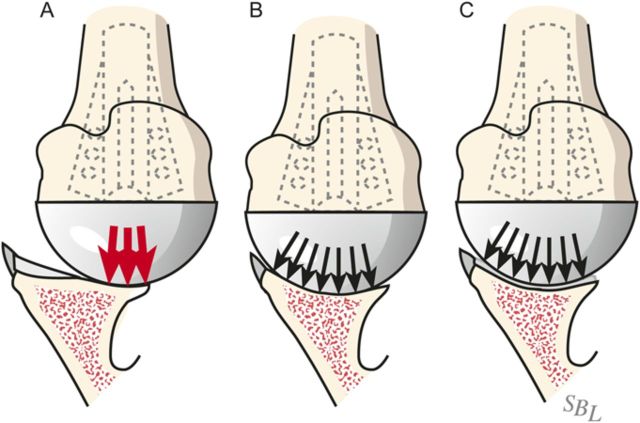
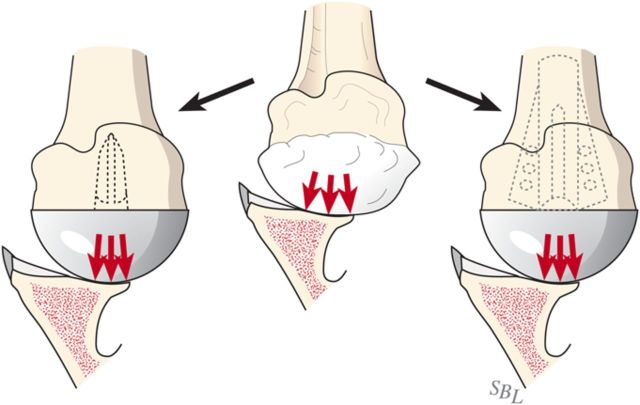
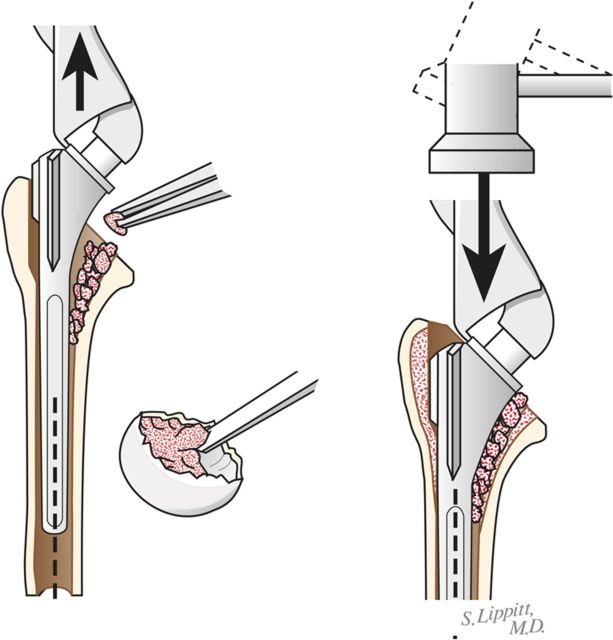
Step 5 humeral prosthesis fixation: Fix the humeral component using impaction autografting.
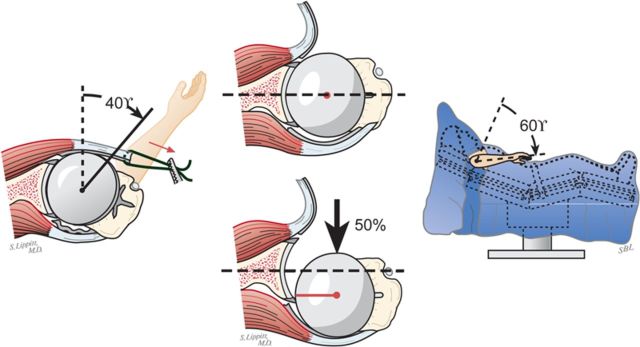
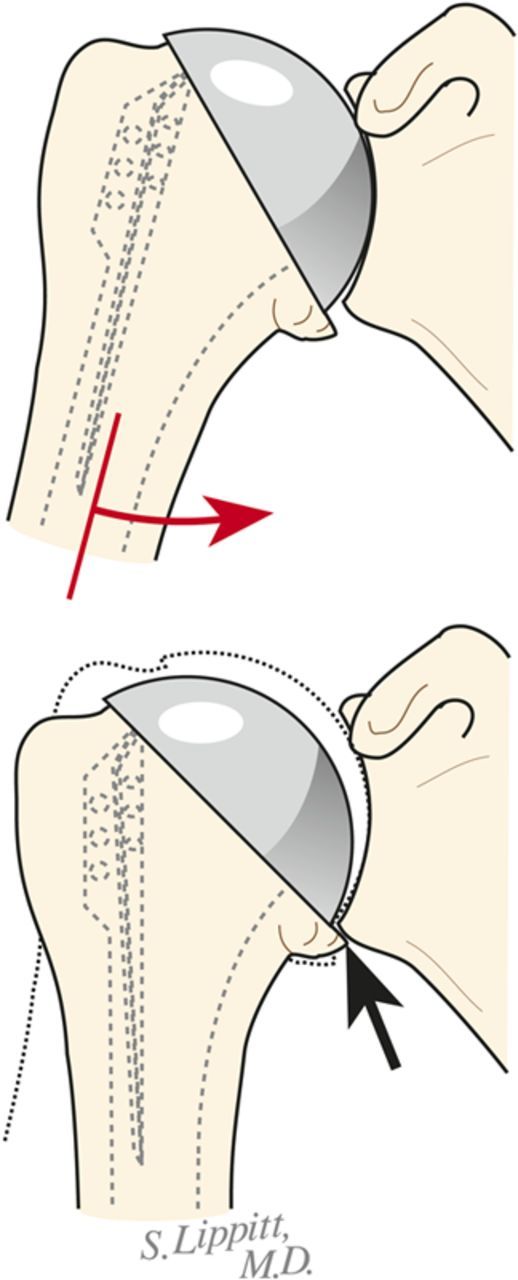
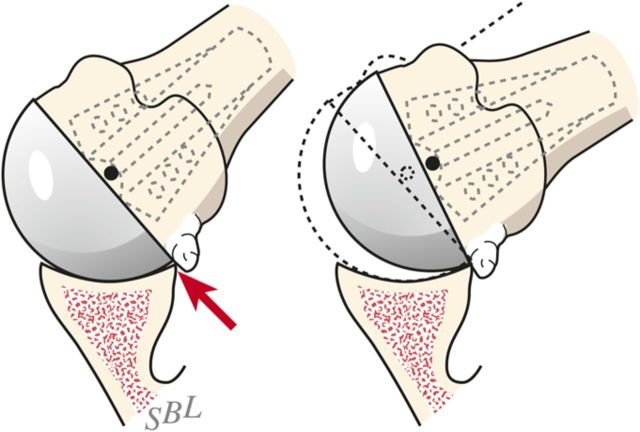
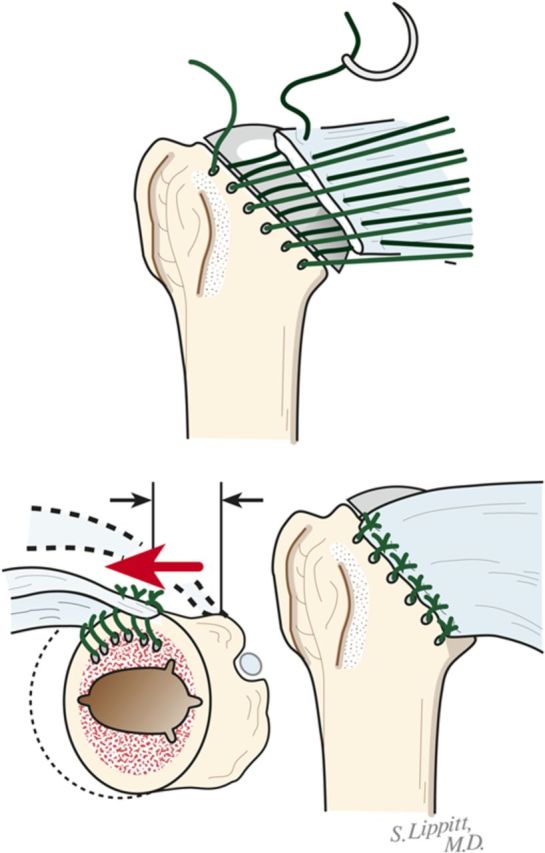
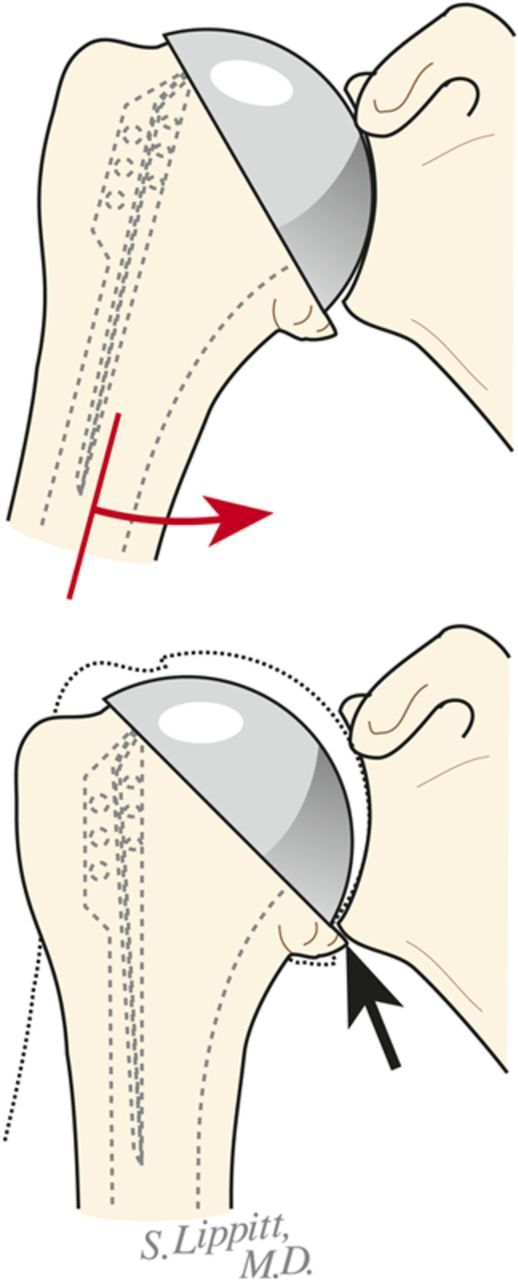
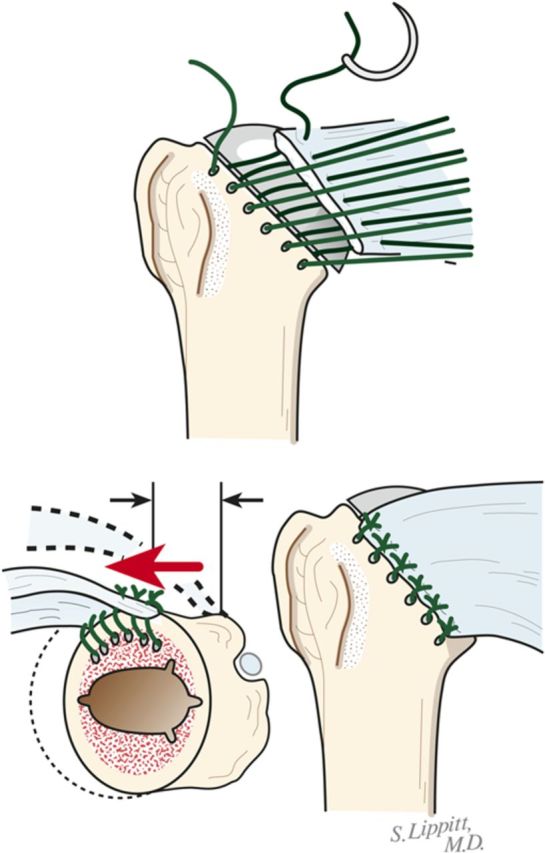
Step 6 soft-tissue balancing: After the definitive humeral prosthesis is in place, ensure the desired balance of mobility and stability. If there is excessive posterior translation, consider a rotator interval plication.
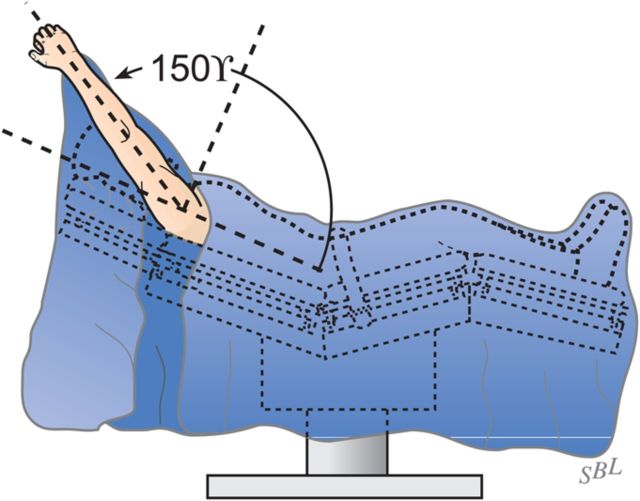
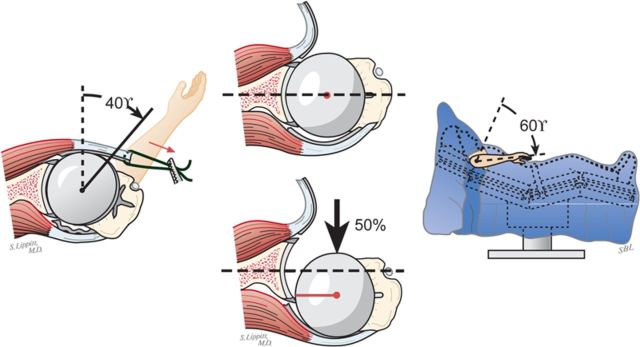
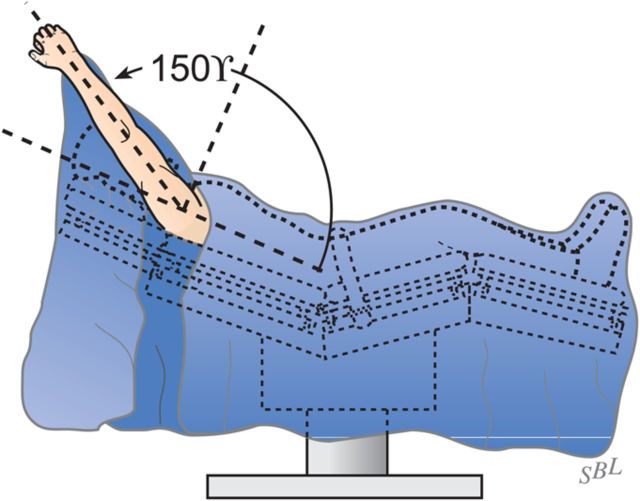
Step 7 rehabilitation: Achieve and maintain at least 150° of flexion and good external rotation strength.
Results: In our study, comfort and function increased progressively after the ream-and-run procedure, reaching a steady state by approximately twenty months.
What to watch for: IndicationsContraindicationsPitfalls & Challenges.
Figures
References
-
- Walch G Young AA Boileau P Loew M Gazielly D Molé D. Patterns of loosening of polyethylene keeled glenoid components after shoulder arthroplasty for primary osteoarthritis: results of a multicenter study with more than five years of follow-up. J Bone Joint Surg Am. 2012 Jan 18;94(2):145-50. - PubMed
-
- Magnussen RA Mallon WJ Willems WJ Moorman CT 3rd. Long-term activity restrictions after shoulder arthroplasty: an international survey of experienced shoulder surgeons. J Shoulder Elbow Surg. 2011 Mar;20(2):281-9. Epub 2010 Nov 4. - PubMed
-
- Matsen FA 3rd. Shoulder arthritis and rotator cuff tears: causes of shoulder pain. Quality information for those concerned with arthritis of the shoulder and rotator cuff pathologies. The ream and run essentials. http://shoulderarthritis.blogspot.com/2012/07/ream-and-run-essentials.html. Accessed 2012 Jul.
-
- Gilmer BB Comstock BA Jette JL Warme WJ Jackins SE Matsen FA III. The prognosis for improvement in comfort and function after the ream-and-run arthroplasty for glenohumeral arthritis. An analysis of 176 consecutive cases. J Bone Joint Surg Am. 2012 Jul 18;94(14):e102. - PubMed
-
- Matsen FA 3rd Clinton J Lynch J Bertelsen A Richardson ML. http://shoulderarthritis.blogspot.com/2012/07/ream-and-run-essentials.html. Accessed 2012 Jul. - PubMed
LinkOut - more resources
Full Text Sources