

Detection and characterisation of optic nerve and retinal changes in primary congenital glaucoma using hand-held optical coherence tomography
- PMID: 31321308
- PMCID: PMC6597657
- DOI: 10.1136/bmjophth-2018-000194
Detection and characterisation of optic nerve and retinal changes in primary congenital glaucoma using hand-held optical coherence tomography
Abstract
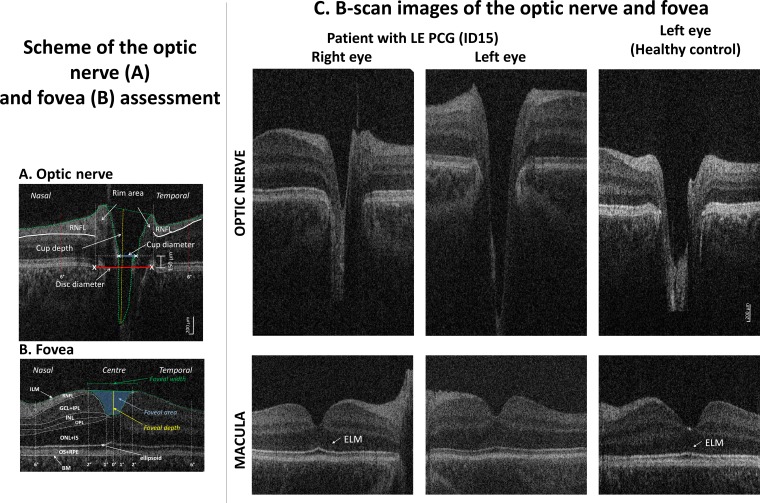
Objective: To investigate (1) the feasibility of scanning the optic nerve (ON) and central retina with hand-held optical coherence tomography (HH-OCT) without sedation or anaesthesia in primary congenital glaucoma (PCG), (2) the characteristics of ON changes in comparison with adult primary open-angle glaucoma (POAG) in comparison with matched controls, (3) the sensitivity and specificity of ON parameters for diagnosis, and (4) changes of foveal morphology.
Methods and analysis: HH-OCT (Envisu 2300; Leica Microsystems) was used to investigate ON and foveal morphology of 20 children with PCG (mean age 4.64±2.79) and 10 adult patients with POAG (mean age 66.8±6.94), and compared with age-matched, gender-matched and ethnicity-matched healthy controls without sedation or anaesthesia.
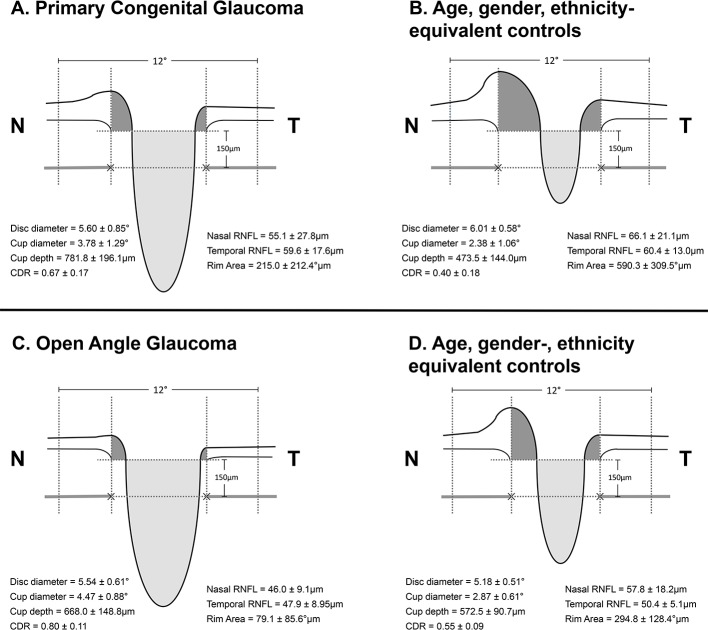
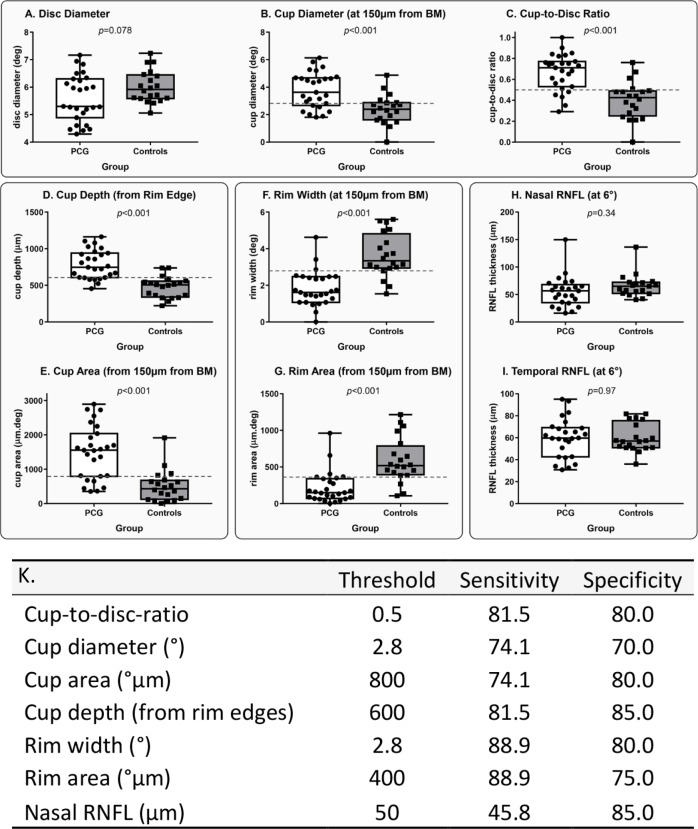
Results: HH-OCT yielded useful data in 20 out of 24 young children with PCG. Patients with PCG had significantly deeper cup changes than patients with POAG (vs respective age-matched controls, p=0.014). ON changes in PCG are characterised by significant increase in cup depth (165%), increased cup diameter (159%) and reduction in rim area (36.4%) as compared with controls with high sensitivity (81.5, 74.1% and 88.9%, respectively) and specificity (85.0, 80.0% and 75.0%, respectively). Patients with PCG have a significantly smaller width of the macula pit (p<0.001) with non-detectable external limiting membrane.
Conclusion: HH-OCT has the potential to be a useful tool in glaucoma management for young children. We have demonstrated the use of HH-OCT in confirming a diagnosis of glaucoma within the studied cohort and found changes in disc morphology which characterise differently in PCG from POAG.
Keywords: child health (paediatrics); diagnostic tests/investigation; imaging.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous