

Relationship between heart rate and optimal reconstruction phase in coronary CT angiography performed on a 256-slice multidetector CT
- PMID: 31322906
- PMCID: PMC6732907
- DOI: 10.1259/bjr.20180945
Relationship between heart rate and optimal reconstruction phase in coronary CT angiography performed on a 256-slice multidetector CT
Abstract
Objective: This study aimed to evaluate the relationship between heart rate (HR) and optimal reconstruction phase in prospectively electrocardiogram (ECG)-triggered coronary CT angiography (CCTA) performed on a newly introduced 256-slice multidetector CT (MDCT).
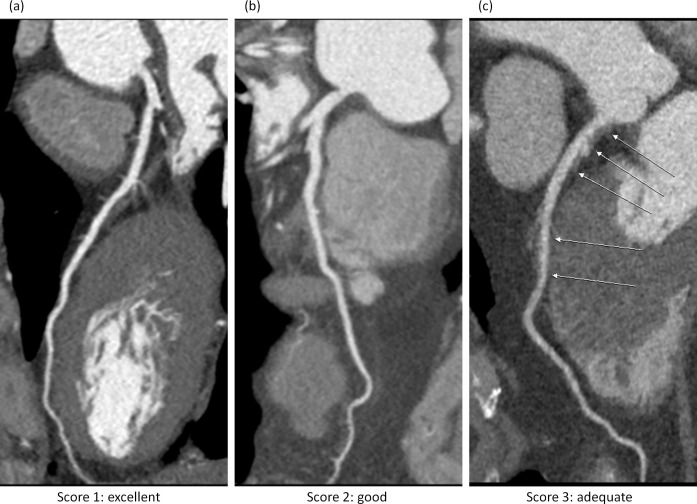
Methods: All the cases were selected retrospectively from the patients scheduled for CCTA in our department between January and April 2017. The scanner selected the optimal exposure phase based on 10 s ECG recordings. To ensure the success of CCTA, the operator also checked patient's age, breathing control, emotional status and past medical history to decide whether the automatically selected scan phase needs manual adjustment or not. Images were reconstructed in 1% steps of the R-R interval to determine the cardiac phase with least coronary motion. If CCTA images showed moderate motion blurring or discontinuity in the course of coronary segments, a cardiac motion correction algorithm was applied to the reconstructed images. Subjective diagnostic image quality was evaluated with 4-point grading scale.
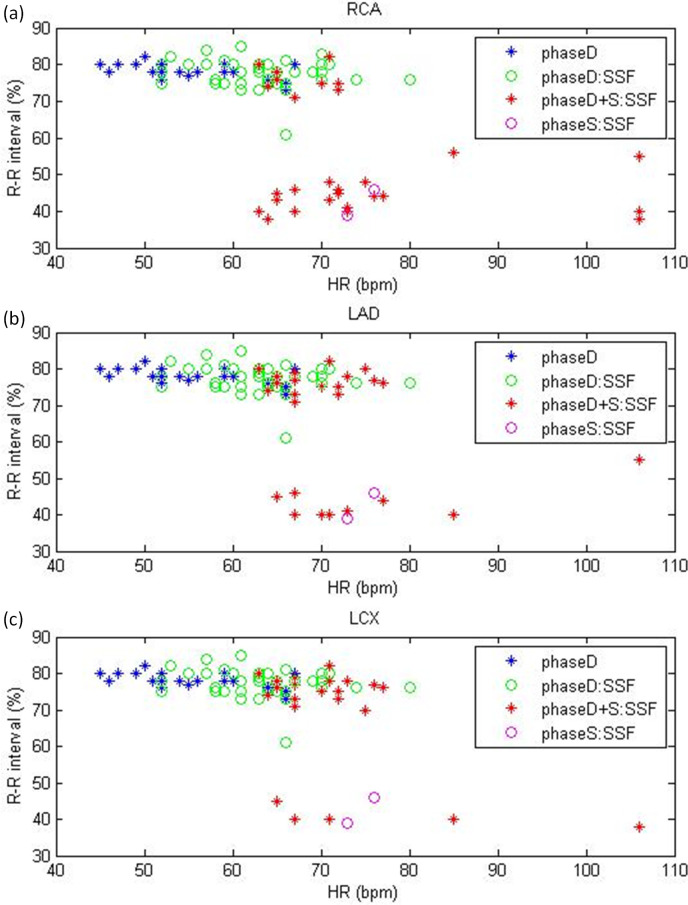
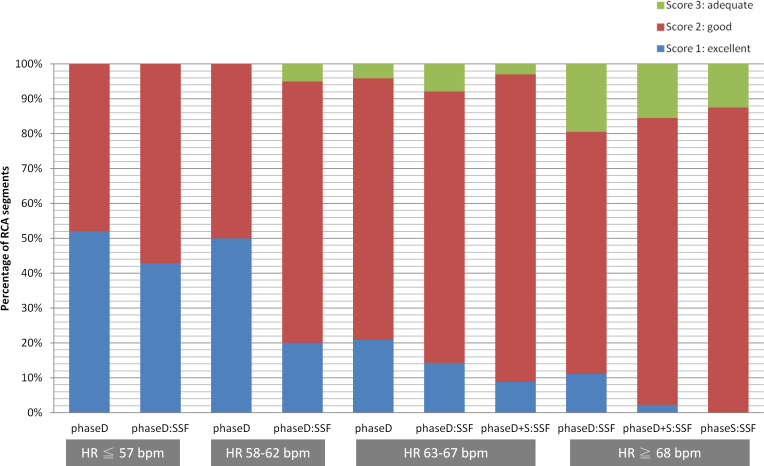
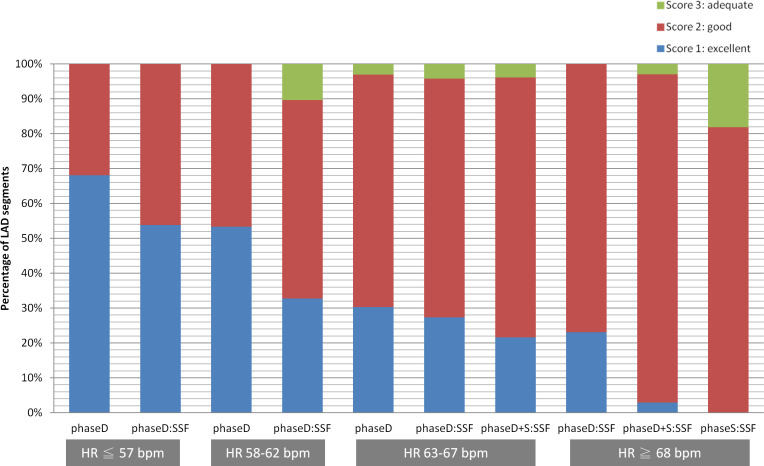
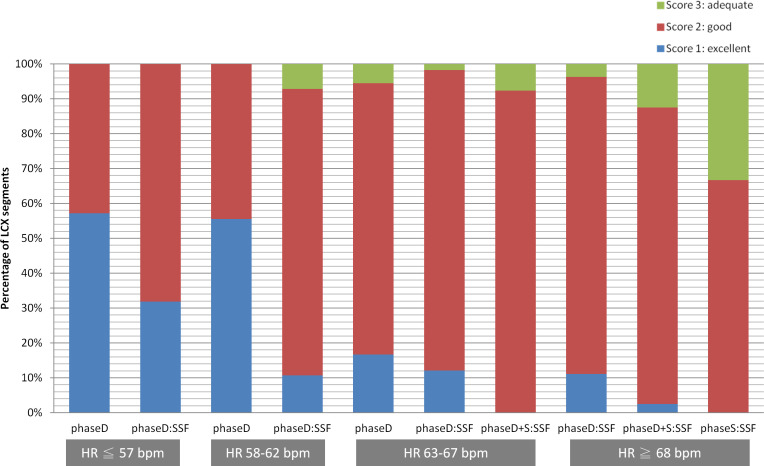
Results: A total of 87 consecutive CCTA examinations were investigated in this study. Diastolic reconstruction was applied to all vessel segments in patients with HR <63 bpm, where 36.5 and 77.8% of vessel segments were reconstructed with the use of motion correction in HR ≤57 and 58-62 bpm, respectively. As for patients with HR ≥63 bpm, 89.3 and 71.7% of vessel segments were reconstructed in diastole in HR 63-67 and ≥68 bpm, respectively, while 81 and 100% of vessel segments were reconstructed with the use of motion correction in the same HR groups.
Conclusion: Based on our results, a HR less than 67 bpm can be used to identify appropriate patients for diastolic reconstruction. Although the motion correction algorithm is an effective approach to reduce the impact of cardiac motion in CCTA, HR control is still important to optimize the image quality of CCTA. The relationship between HR and optimal reconstruction phase established in this study could be further used to tailor the ECG pulsing window for dose reduction in patients undergoing CCTA performed on the 256-slice MDCT.
Advances in knowledge: The HR thresholds to identify patients who are the best suitable candidates for diastolic or systolic reconstruction are scanner specific. This study investigated the relationship between HR and optimal reconstruction phase in prospectively ECG-triggered CCTA for a newly introduced 256-slice MDCT. Once the relationship is established, it could be used to tailor the ECG pulsing window for radiation dose reduction.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
