

A Narrative Review of Cancer-Related Fatigue (CRF) and Its Possible Pathogenesis
- PMID: 31323874
- PMCID: PMC6679212
- DOI: 10.3390/cells8070738
A Narrative Review of Cancer-Related Fatigue (CRF) and Its Possible Pathogenesis
Abstract
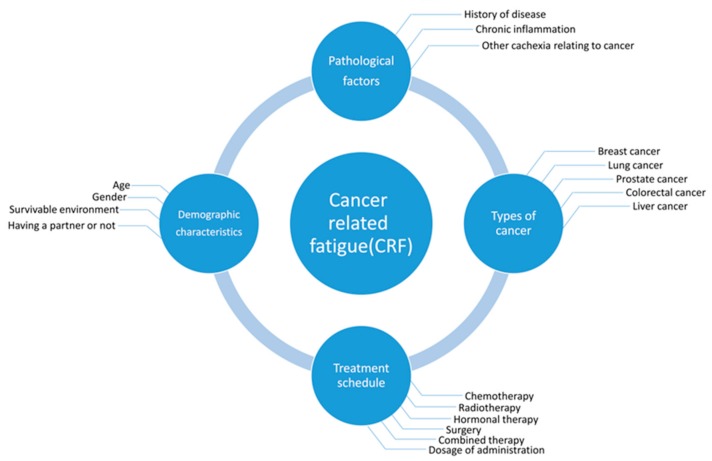
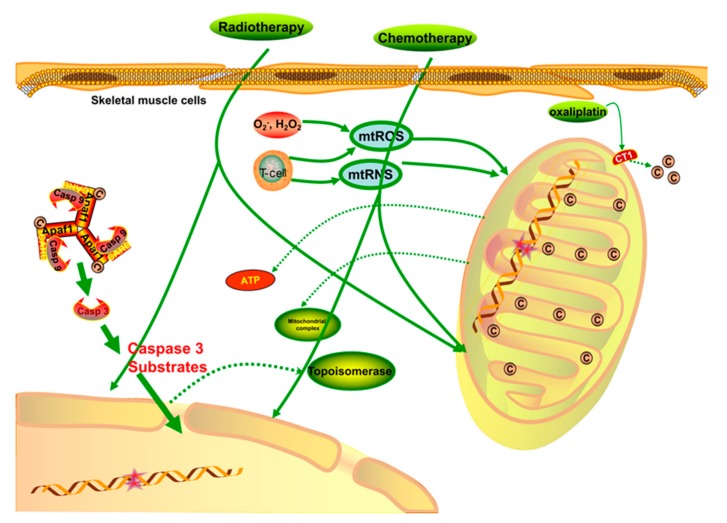
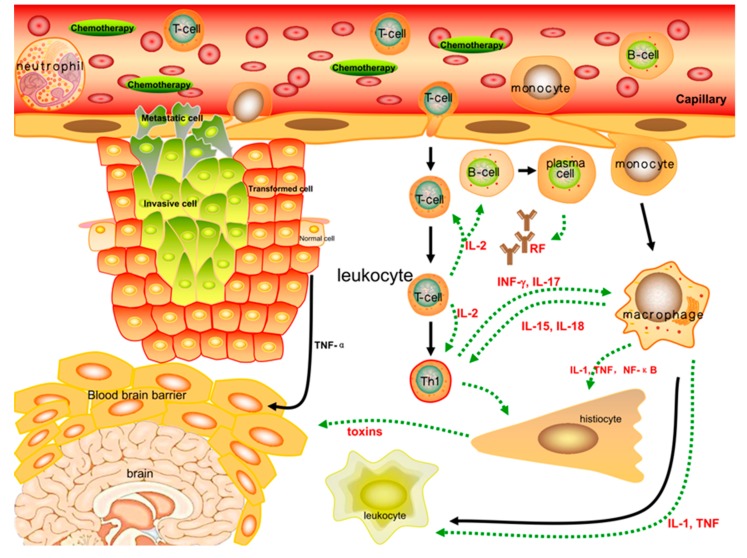
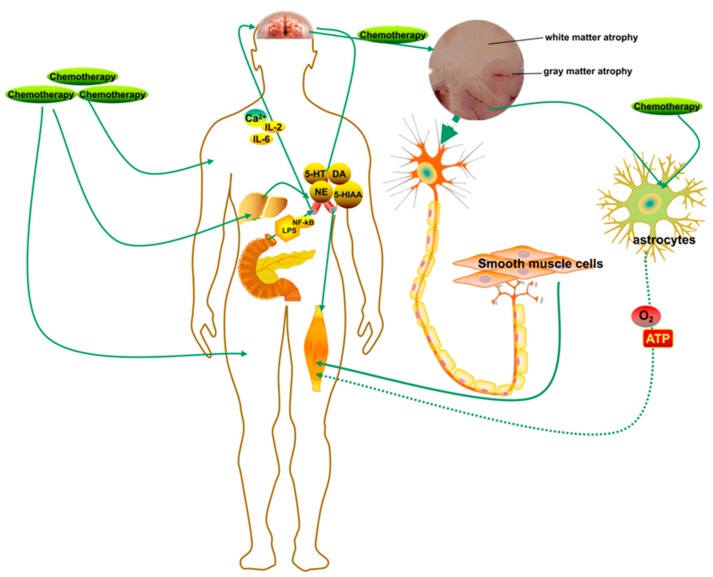
Many cancer patients suffer from severe fatigue when treated with chemotherapy or radiotherapy; however, the etiology and pathogenesis of this kind of fatigue remains unknown. Fatigue is associated with cancer itself, as well as adjuvant therapies and can persist for a long time. Cancer patients present a high degree of fatigue, which dramatically affects the quality of their everyday life. There are various clinical research studies and reviews that aimed to explore the mechanisms of cancer-related fatigue (CRF). However, there are certain limitations in these studies: For example, some studies have only blood biochemical texts without histopathological examination, and there has been insufficient systemic evaluation of the dynamic changes in relevant indexes. Thus, we present this narrative review to summarize previous studies on CRF and explore promising research directions. Plenty of evidence suggests a possible association between CRF and physiological dysfunction, including skeletal muscular and mitochondrial dysfunction, peripheral immune activation and inflammation dysfunction, as well as central nervous system (CNS) disorder. Mitochondrial DNA (mtDNA), mitochondrial structure, oxidative pressure, and some active factors such as ATP play significant roles that lead to the induction of CRF. Meanwhile, several pro-inflammatory and anti-inflammatory cytokines in the peripheral system, even in the CNS, significantly contribute to the occurrence of CRF. Moreover, CNS function disorders, such as neuropeptide, neurotransmitter, and hypothalamic-pituitary-adrenal (HPA) axis dysfunction, tend to amplify the sense of fatigue in cancer patients through various signaling pathways. There have been few accurate animal models established to further explore the molecular mechanisms of CRF due to different types of cancer, adjuvant therapy schedules, living environments, and physical status. It is imperative to develop appropriate animal models that can mimic human CRF and to explore additional mechanisms using histopathological and biochemical methods. Therefore, the main purpose of this review is to analyze the possible pathogenesis of CRF and recommend future research that will clarify CRF pathogenesis and facilitate the formulation of new treatment options.
Keywords: cancer-related fatigue; central nervous system; inflammatory cytokines; mitochondrion; peripheral immune activation; skeletal muscle.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yancey J.R., Thomas S.M. Chronic fatigue syndrome: Diagnosis and treatment. Am. Fam. Physician. 2012;86:741–746. - PubMed
-
- Hawley J.A., Reilly T. Fatigue revisited. J. Sports Sci. 1997;15:245–246. - PubMed
-
- Cancer-related fatigue. Clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2003;1:308–331. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
