

High-Risk Multiple Myeloma: Integrated Clinical and Omics Approach Dissects the Neoplastic Clone and the Tumor Microenvironment
- PMID: 31323969
- PMCID: PMC6678140
- DOI: 10.3390/jcm8070997
High-Risk Multiple Myeloma: Integrated Clinical and Omics Approach Dissects the Neoplastic Clone and the Tumor Microenvironment
Abstract
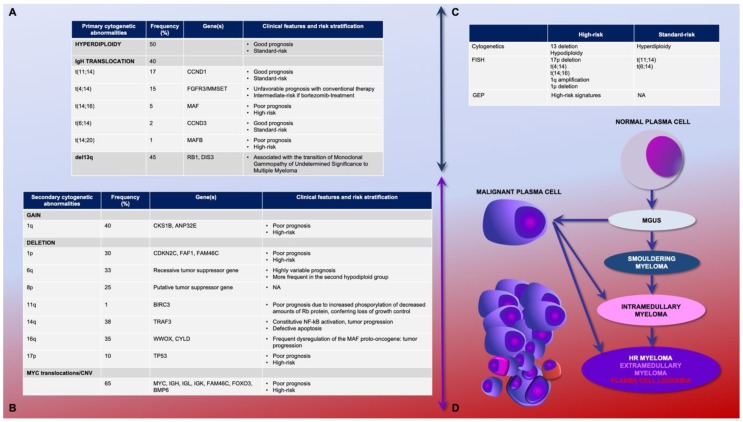
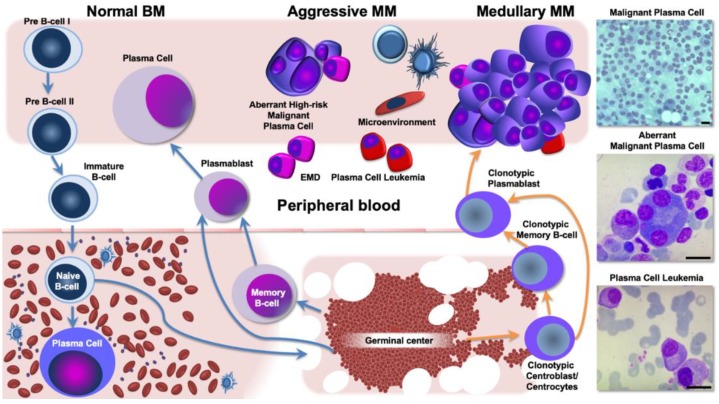
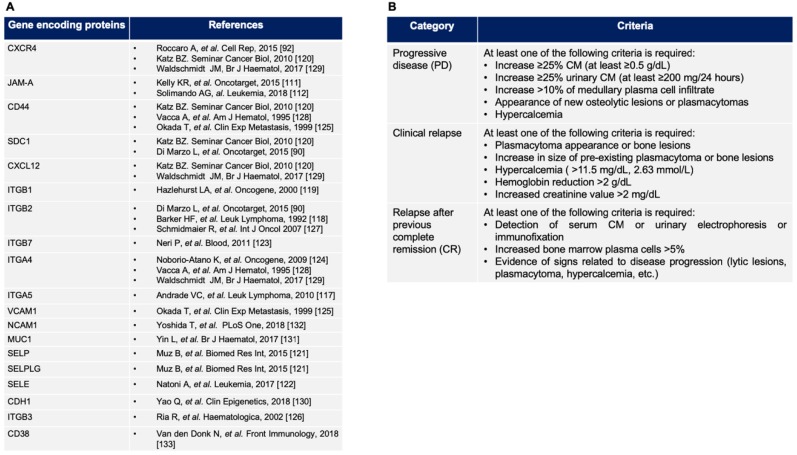
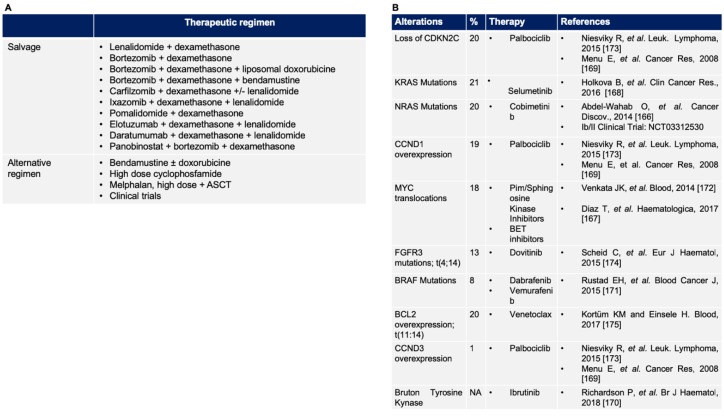
Multiple myeloma (MM) is a genetically heterogeneous disease that includes a subgroup of 10-15% of patients facing dismal survival despite the most intensive treatment. Despite improvements in biological knowledge, MM is still an incurable neoplasia, and therapeutic options able to overcome the relapsing/refractory behavior represent an unmet clinical need. The aim of this review is to provide an integrated clinical and biological overview of high-risk MM, discussing novel therapeutic perspectives, targeting the neoplastic clone and its microenvironment. The dissection of the molecular determinants of the aggressive phenotypes and drug-resistance can foster a better tailored clinical management of the high-risk profile and therapy-refractoriness. Among the current clinical difficulties in MM, patients' management by manipulating the tumor niche represents a major challenge. The angiogenesis and the stromal infiltrate constitute pivotal mechanisms of a mutual collaboration between MM and the non-tumoral counterpart. Immuno-modulatory and anti-angiogenic therapy hold great efficacy, but variable and unpredictable responses in high-risk MM. The comprehensive understanding of the genetic heterogeneity and MM high-risk ecosystem enforce a systematic bench-to-bedside approach. Here, we provide a broad outlook of novel druggable targets. We also summarize the existing multi-omics-based risk profiling tools, in order to better select candidates for dual immune/vasculogenesis targeting.
Keywords: angiogenesis; bone marrow microenvironment; drug resistance; extramedullary disease; multiple myeloma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kumar S.K., Dispenzieri A., Lacy M.Q., Gertz M.A., Buadi F.K., Pandey S., Kapoor P., Dingli D., Hayman S.R., Leung N., et al. Continued improvement in survival in multiple myeloma: Changes in early mortality and outcomes in older patients. Leukemia. 2014;28:1122–1128. doi: 10.1038/leu.2013.313. - DOI - PMC - PubMed
-
- Sonneveld P., Avet-Loiseau H., Lonial S., Usmani S., Siegel D., Anderson K.C., Chng W.J., Moreau P., Attal M., Kyle R.A., et al. Treatment of multiple myeloma with high-risk cytogenetics: A consensus of the International Myeloma Working Group. Blood. 2016;127:2955–2962. doi: 10.1182/blood-2016-01-631200. - DOI - PMC - PubMed
