

Implications of Early Decline in eGFR due to Intensive BP Control for Cardiovascular Outcomes in SPRINT
- PMID: 31324734
- PMCID: PMC6683716
- DOI: 10.1681/ASN.2018121261
Implications of Early Decline in eGFR due to Intensive BP Control for Cardiovascular Outcomes in SPRINT
Abstract
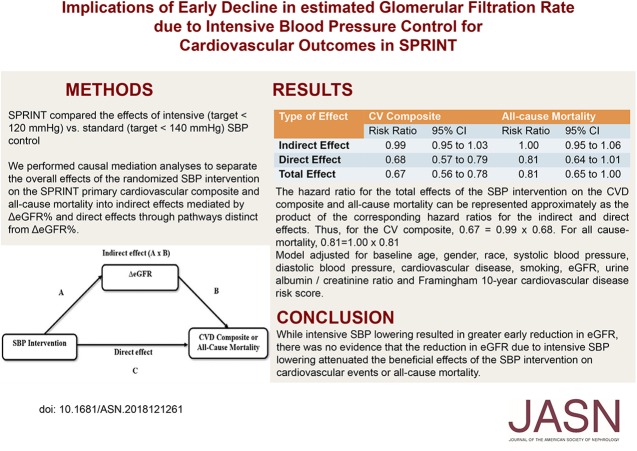
Background: The Systolic BP Intervention Trial (SPRINT) found that intensive versus standard systolic BP control (targeting <120 or <140 mm Hg, respectively) reduced the risks of death and major cardiovascular events in persons with elevated cardiovascular disease risk. However, the intensive intervention was associated with an early decline in eGFR, and the clinical implications of this early decline are unclear.
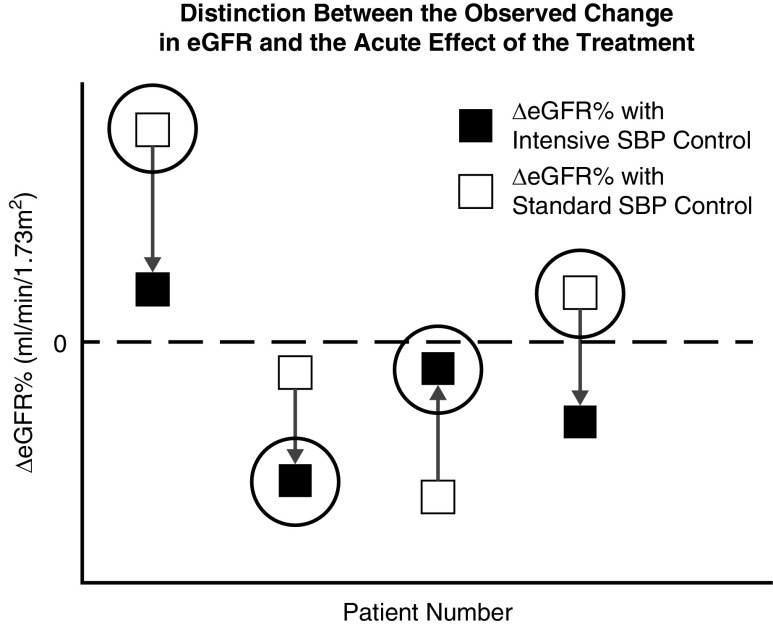
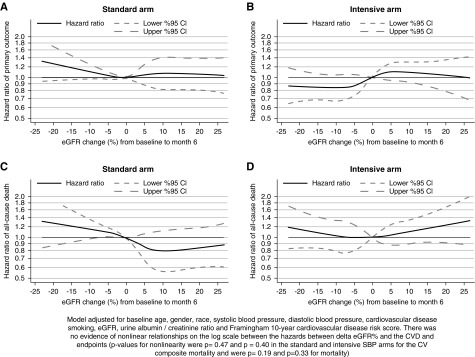
Methods: In a post hoc analysis of SPRINT, we defined change in eGFR as the percentage change in eGFR at 6 months compared with baseline. We performed causal mediation analyses to separate the overall effects of the randomized systolic BP intervention on the SPRINT primary cardiovascular composite and all-cause mortality into indirect effects (mediated by percentage change in eGFR) and direct effects (mediated through pathways other than percentage change in eGFR).
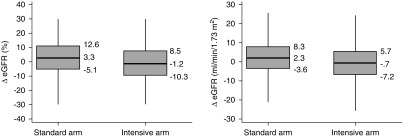
Results: About 10.3% of the 4270 participants in the intensive group had a ≥20% eGFR decline versus 4.4% of the 4256 participants in the standard arm (P<0.001). After the 6-month visit, there were 591 cardiovascular composite events during 27,849 person-years of follow-up. The hazard ratios for total effect, direct effect, and indirect effect of the intervention on the cardiovascular composite were 0.67 (95% confidence interval [95% CI], 0.56 to 0.78), 0.68 (95% CI, 0.57 to 0.79), and 0.99 (95% CI, 0.95 to 1.03), respectively. All-cause mortality results were similar.
Conclusions: Although intensive systolic BP lowering resulted in greater early decline in eGFR, there was no evidence that the reduction in eGFR owing to intensive systolic BP lowering attenuated the beneficial effects of this intervention on cardiovascular events or all-cause mortality.
Keywords: cardiovascular disease; hypertension; mortality; renal hemodynamics.
Copyright © 2019 by the American Society of Nephrology.
Figures

References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration : Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 360: 1903–1913, 2002 - PubMed
-
- Hsu CY, McCulloch CE, Darbinian J, Go AS, Iribarren C: Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch Intern Med 165: 923–928, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- R21 HL145494/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- R01 DK118219/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- C06 RR011234/RR/NCRR NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- R21 DK106574/DK/NIDDK NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
