

A rule-based method for predicting the electrical activation of the heart with cardiac resynchronization therapy from non-invasive clinical data
- PMID: 31326854
- PMCID: PMC6746621
- DOI: 10.1016/j.media.2019.06.017
A rule-based method for predicting the electrical activation of the heart with cardiac resynchronization therapy from non-invasive clinical data
Abstract
Background: Cardiac Resynchronization Therapy (CRT) is one of the few effective treatments for heart failure patients with ventricular dyssynchrony. The pacing location of the left ventricle is indicated as a determinant of CRT outcome.
Objective: Patient specific computational models allow the activation pattern following CRT implant to be predicted and this may be used to optimize CRT lead placement.
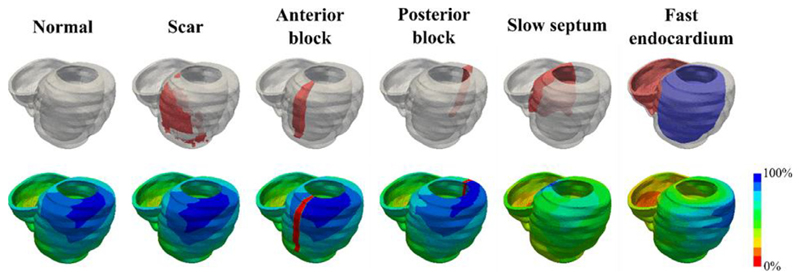
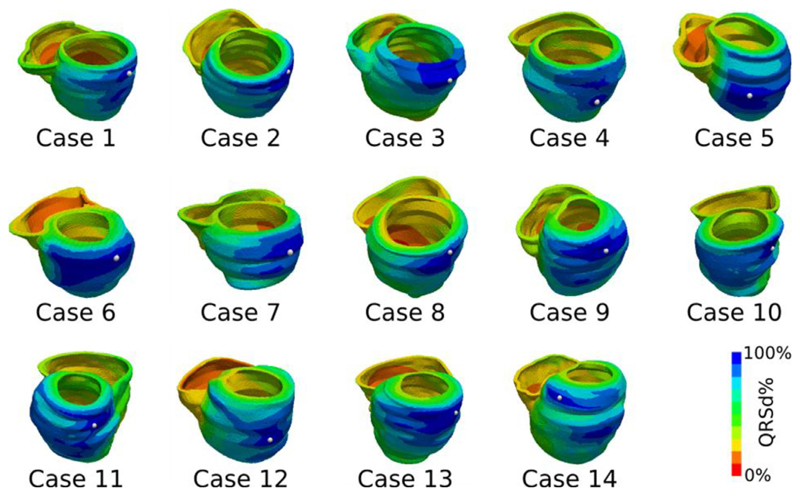
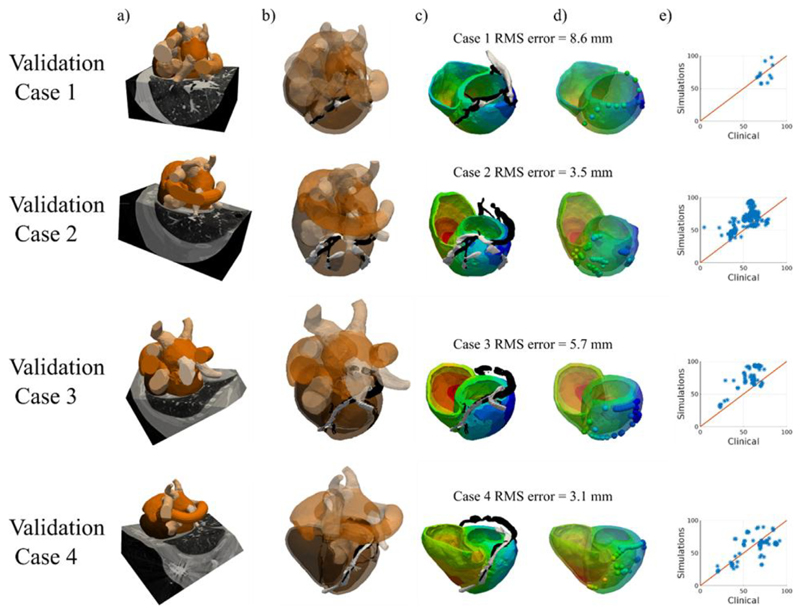
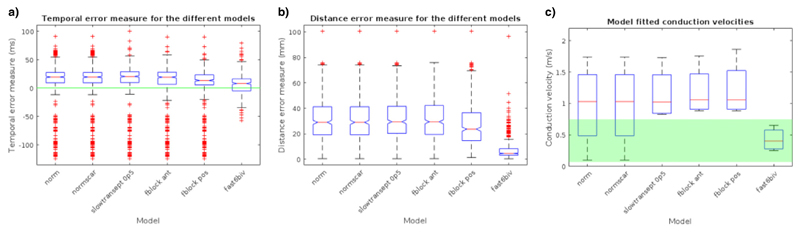
Methods: In this study, the effects of heterogeneous cardiac substrate (scar, fast endocardial conduction, slow septal conduction, functional block) on accurately predicting the electrical activation of the LV epicardium were tested to determine the minimal detail required to create a rule based model of cardiac electrophysiology. Non-invasive clinical data (CT or CMR images and 12 lead ECG) from eighteen patients from two centers were used to investigate the models.
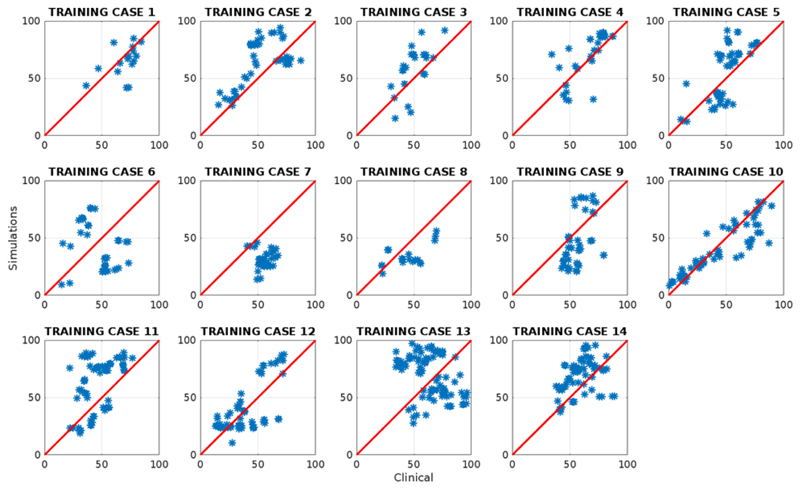
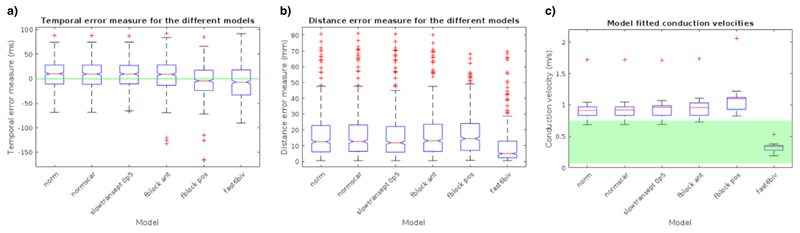
Results: Validation with invasive electro-anatomical mapping data identified that computer models with fast endocardial conduction were able to predict the electrical activation with a mean distance errors of 9.2 ± 0.5 mm (CMR data) or (CT data) 7.5 ± 0.7 mm.
Conclusion: This study identified a simple rule-based fast endocardial conduction model, built using non-invasive clinical data that can be used to rapidly and robustly predict the electrical activation of the heart. Pre-procedural prediction of the latest electrically activating region to identify the optimal LV pacing site could potentially be a useful clinical planning tool for CRT procedures.
Keywords: Cardiac resynchronization therapy; Computational models; Electrophysiology; Patient-specific simulations.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
None.
Figures
References
-
- Akar FG, Spragg DD, Tunin RS, Kass DA, Tomaselli GF. Mechanisms underlying conduction slowing and arrhythmogenesis in nonischemic dilated cardiomyopathy. Circ Res. 2004;95:717–725. - PubMed
-
- Auricchio A, Fantoni C, Regoli F, Carbucicchio C, Goette A, Geller C, Kloss M, Klein H. Characterization of left ventricular activation in patients with heart failure and left bundle-branch block. Circulation. 2004;109:1133–1139. - PubMed
-
- Berruezo A, Mont L, Nava S, Chueca E, Bartholomay E, Brugada J. Electrocardiographic recognition of the epicardial origin of ventricular tachycardias. Circulation. 2004;109:1842–1847. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
