

Preventing dementia by preventing stroke: The Berlin Manifesto
- PMID: 31327392
- PMCID: PMC7001744
- DOI: 10.1016/j.jalz.2019.06.001
Preventing dementia by preventing stroke: The Berlin Manifesto
Abstract
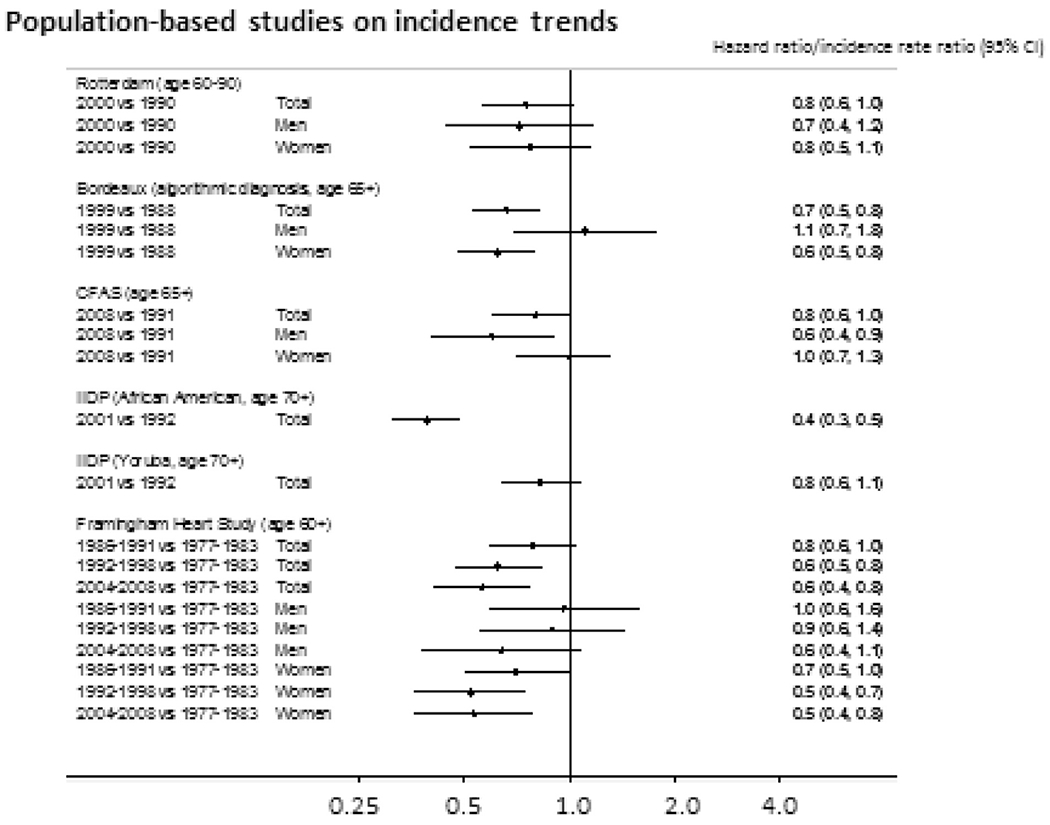
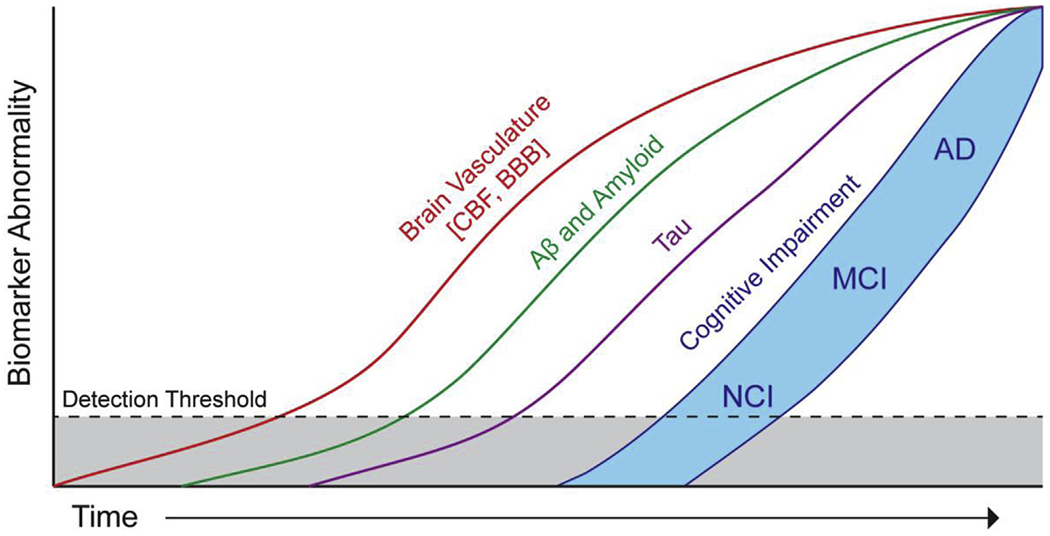
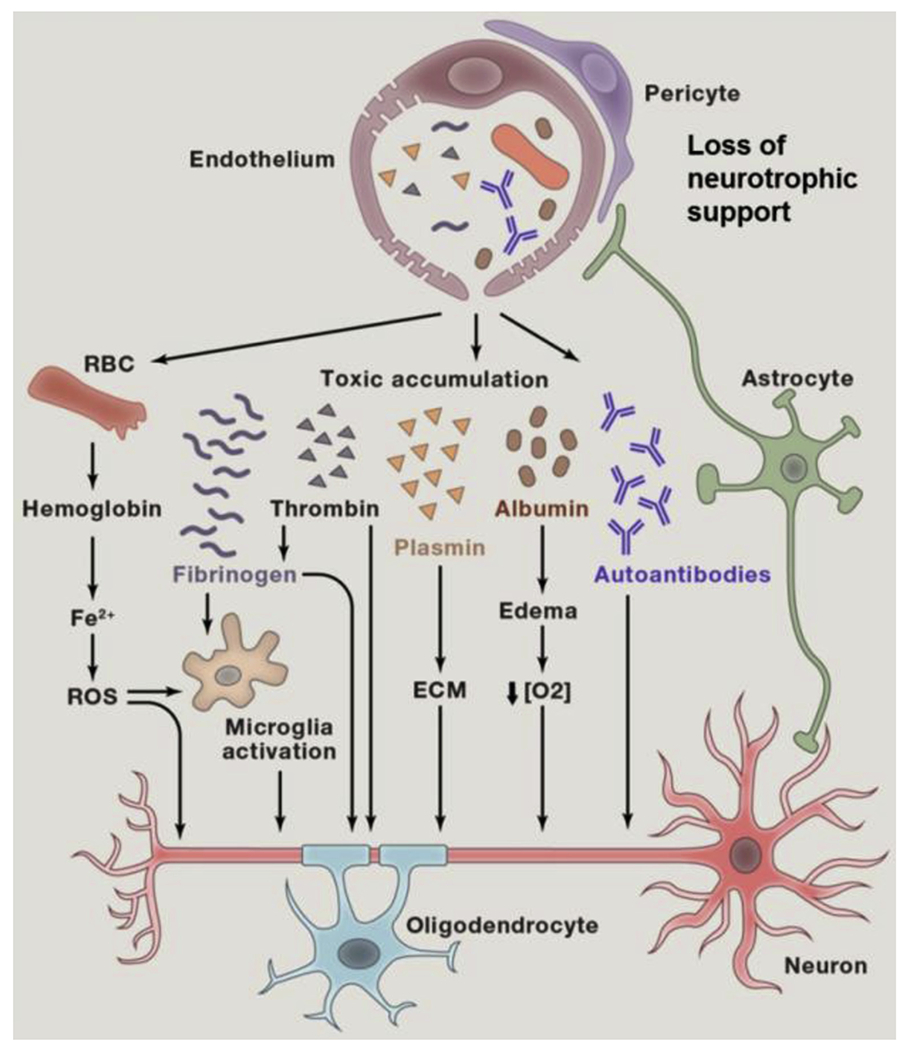
The incidence of stroke and dementia are diverging across the world, rising for those in low- and middle-income countries and falling in those in high-income countries. This suggests that whatever factors cause these trends are potentially modifiable. At the population level, neurological disorders as a group account for the largest proportion of disability-adjusted life years globally (10%). Among neurological disorders, stroke (42%) and dementia (10%) dominate. Stroke and dementia confer risks for each other and share some of the same, largely modifiable, risk and protective factors. In principle, 90% of strokes and 35% of dementias have been estimated to be preventable. Because a stroke doubles the chance of developing dementia and stroke is more common than dementia, more than a third of dementias could be prevented by preventing stroke. Developments at the pathological, pathophysiological, and clinical level also point to new directions. Growing understanding of brain pathophysiology has unveiled the reciprocal interaction of cerebrovascular disease and neurodegeneration identifying new therapeutic targets to include protection of the endothelium, the blood-brain barrier, and other components of the neurovascular unit. In addition, targeting amyloid angiopathy aspects of inflammation and genetic manipulation hold new testable promise. In the meantime, accumulating evidence suggests that whole populations experiencing improved education, and lower vascular risk factor profiles (e.g., reduced prevalence of smoking) and vascular disease, including stroke, have better cognitive function and lower dementia rates. At the individual levels, trials have demonstrated that anticoagulation of atrial fibrillation can reduce the risk of dementia by 48% and that systolic blood pressure lower than 140 mmHg may be better for the brain. Based on these considerations, the World Stroke Organization has issued a proclamation, endorsed by all the major international organizations focused on global brain and cardiovascular health, calling for the joint prevention of stroke and dementia. This article summarizes the evidence for translation into action.
Keywords: Alzheimer's disease; Cognitive impairment; Dementia; Neurovascular unit; Policy; Prevention; Resilience; Risk factor reduction; Stroke; Treatment.
Copyright © 2019 the Alzheimer's Association and the World Stroke Organisation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial Berlin Manifesto October.Int J Stroke. 2019 Oct;14(7):669. doi: 10.1177/1747493019884260. Int J Stroke. 2019. PMID: 31657285 No abstract available.
References
-
- O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010;376:112–23. - PubMed
-
- Feigin VL. Global burden of stroke and risk factors in 188 countries, during 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol 2016;15:913–24. - PubMed
-
- Hachinski V. Dementia: Paradigm shifting into high gear. Alzheimers Dement 2019;15:985–94. - PubMed
Publication types
MeSH terms
Grants and funding
- MR/J006971/1/MRC_/Medical Research Council/United Kingdom
- P50 AG005142/AG/NIA NIH HHS/United States
- R01 NS037853/NS/NINDS NIH HHS/United States
- R01 NS100447/NS/NINDS NIH HHS/United States
- R01 NS034179/NS/NINDS NIH HHS/United States
- G1001245/MRC_/Medical Research Council/United Kingdom
- R380R/1114/DMT_/The Dunhill Medical Trust/United Kingdom
- CS/15/5/31475/BHF_/British Heart Foundation/United Kingdom
- G0701120/MRC_/Medical Research Council/United Kingdom
- MR/L023784/2/MRC_/Medical Research Council/United Kingdom
- P01 AG052350/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
