

Family-focused cognitive behavioral treatment for depressed adolescents in suicidal crisis with co-occurring risk factors: a randomized trial
- PMID: 31328281
- PMCID: PMC6742562
- DOI: 10.1111/jcpp.13095
Family-focused cognitive behavioral treatment for depressed adolescents in suicidal crisis with co-occurring risk factors: a randomized trial
Abstract
Background: Suicide is the second leading cause of death among adolescents. The purpose of this study was to test a family-focused outpatient cognitive behavioral treatment (F-CBT) protocol for depressed adolescents following psychiatric hospitalization for a suicide attempt or suicidal ideation, and who had a co-occurring risk factor (suicidal behavior prior to the index admission, nonsuicidal self-injury, and/or a substance use disorder), in a randomized Phase 2 efficacy trial.
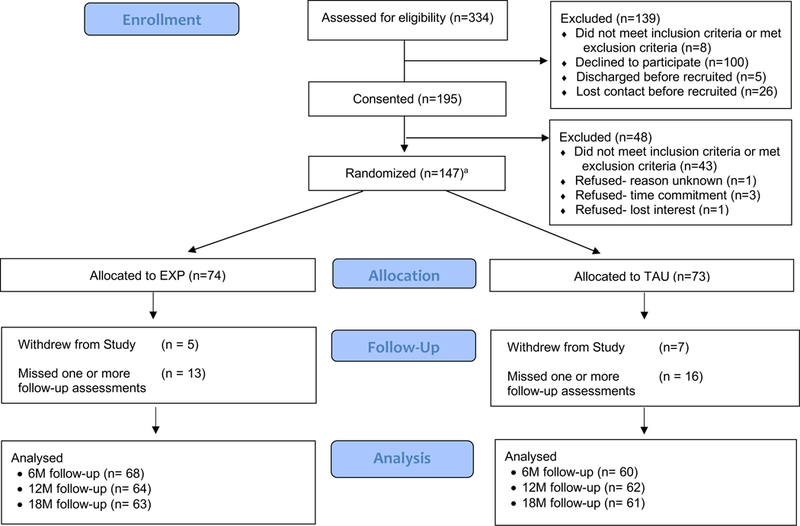
Method: One hundred forty-seven adolescents (mean age = 14.91 years; 76.2% female, 85.5% White) and their families, recruited primarily from an inpatient psychiatric hospitalization program, were randomly assigned to F-CBT or enhanced treatment-as-usual (E-TAU). A suicide attempt was the primary outcome variable. Depression, suicidal ideation, and nonsuicidal self-injury are also reported here. Assessments were completed at pretreatment as well as 6, 12, and 18-months postrandomization (Trial Registration ClinicalTrials.gov Identifier: NCT01732601).
Results: In the sample as a whole, rates of attempts decreased from 20% at 6 months to 9% at 12 months to 7% at 18 months. There was no evidence of a significant difference between treatment arms in rates of suicide attempts, major depressive disorder, suicidal ideation, or nonsuicidal self-injury at any of the postrandomization assessment points.
Conclusions: Though F-CBT was associated with reductions in suicidality, depression, and nonsuicidal self-injury, E-TAU showed an equally strong effect. Greater frequency of F-CBT treatment sessions, particularly at the start of care, and alternative approaches to transitioning to care at 12 months, may be necessary when using F-CBT with this population.
Keywords: Suicide; adolescent; clinical trial; cognitive behavioral therapy.
© 2019 Association for Child and Adolescent Mental Health.
Conflict of interest statement
Conflict of interest statement: No conflicts declared.
The authors have declared that they have no competing or potential conflicts of interest.
Figures
References
-
- Burns B, Angold A, Magruder-Habib K, Costello E, Patrick M (1997). Child and Adolescent Services Assessment (version 4.2). Durham, NC: Duke University.
-
- Centers for Disease Control and Prevention. Web-Based Injury Statistics Query and Reporting System (WISQARS). Atlanta, GA: Centers for Disease Control and Prevention; 2017. http://www.cdc.gov/injury/wisqars/LeadingCauses.html
-
- Cigularov K, Chen PY, Thurber BW, & Stallones L (2008). What prevents adolescents from seeking help after a suicide education program? Suicide and Life-Threatening Behavior, 38, 74–86. - PubMed
-
- Curtin SC, Hedegaard H, Minino AM, Warner M QuickStats: Death rates for motor vehicle traffic injury, suicide, and homicide among children and adolescents aged 10–14 years — United States, 1999–2014. MMWR Morb Mortal Wkly Rep. 2016;65. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
