

Association Between Stress Testing-Induced Myocardial Ischemia and Clinical Events in Patients With Multivessel Coronary Artery Disease
- PMID: 31329221
- PMCID: PMC6647357
- DOI: 10.1001/jamainternmed.2019.2227
Association Between Stress Testing-Induced Myocardial Ischemia and Clinical Events in Patients With Multivessel Coronary Artery Disease
Abstract
Importance: The long-term prognostic implications of myocardial ischemia documented during stress testing in patients with multivessel coronary artery disease (CAD) are unclear.
Objective: To assess whether documented stress testing-induced myocardial ischemia is associated with major adverse cardiovascular events or ventricular function changes in patients with stable multivessel CAD.
Design, setting, and participants: A prospective cohort study was conducted using data from a single-center randomized clinical trial (Medicine, Angioplasty, or Surgery Study [MASS] II) to examine the association of myocardial ischemia documented during stress testing at baseline with cardiovascular events and ventricular function changes during follow-up. Participants were previously randomized (May 1, 1995, to May 31, 2000) to medical therapy, percutaneous coronary intervention with bare metal stents, or coronary artery bypass grafting. Event-free survival was estimated by the Kaplan-Meier method, and multivariable Cox regression models were calculated to assess the association between ischemia and the primary composite end point. The vital status was determined on February 28, 2011. Data were analyzed from February 1, 2016, to April 1, 2017.
Main outcomes and measures: Cardiovascular events (overall mortality, myocardial infarction, and revascularization for refractory angina) were tracked from the time of randomization to the end of the 10-year follow-up (mean [SD] duration, 11.4 [4.3] years). Myocardial ischemia was assessed at baseline and at 1-year intervals by exercise stress testing, and ventricular function (left ventricular ejection fraction) was assessed by echocardiography at baseline and after 10 years. Patients with documented ischemia were compared with those without ischemia regarding the outcomes and changes in ventricular function.
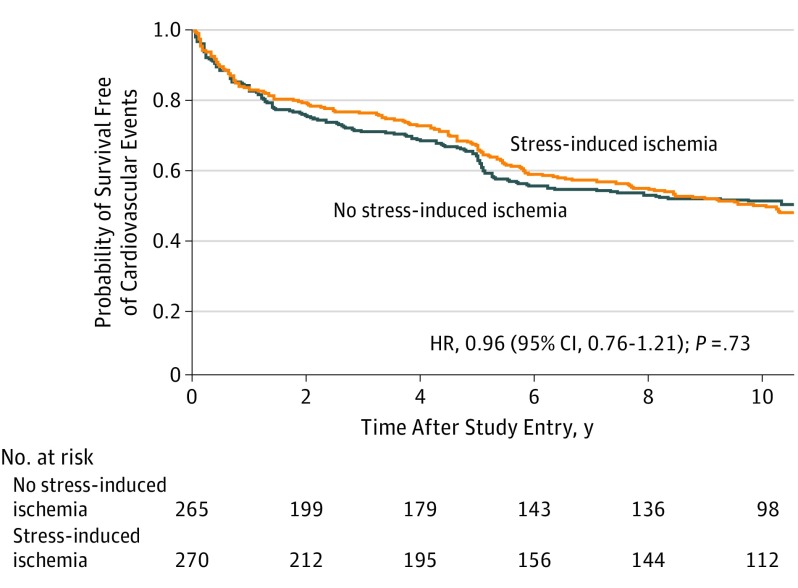
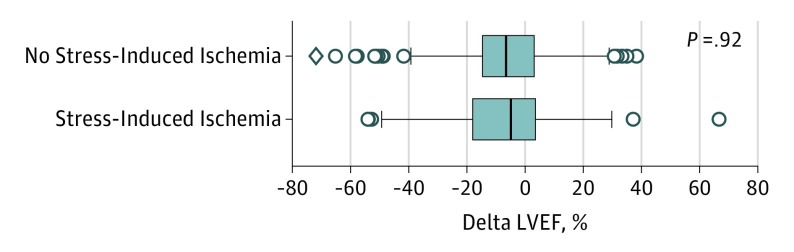
Results: Of 611 participants, 535 underwent exercise stress testing at baseline: 270 with documented ischemia and 265 without. Of these 535 patients, 373 (69.7%) were men, and the mean (SD) age for the entire cohort was 59.7 (9.2) years. No association was found between the presence of ischemia at baseline and survival free of combined cardiovascular events (hazard ratio, 1.00; 95% CI, 0.80-1.27; P = .95) after multivariable adjustment that included CAD initial randomized treatments. In addition, among 320 patients who underwent echocardiographic evaluation, the slight decline in left ventricular ejection fraction after 10 years was similar in both groups (median [SD] difference, -4.9% [18.7%] vs -6.6% [20.0%], respectively, for groups with and without ischemia; P = .97).
Conclusions and relevance: In this study, regardless of the therapeutic strategy applied, the presence of documented myocardial ischemia did not appear to be associated with an increased occurrence of major adverse cardiovascular events or changes in ventricular function in patients with multivessel CAD during a long-term follow-up.
Conflict of interest statement
Figures
Comment in
-
Stress Testing and Risk Prediction in People With Known Symptomatic Multivessel Coronary Artery Disease.JAMA Intern Med. 2020 Jan 1;180(1):165-166. doi: 10.1001/jamainternmed.2019.5854. JAMA Intern Med. 2020. PMID: 31904787 No abstract available.
-
Stress Testing and Risk Prediction in People With Known Symptomatic Multivessel Coronary Artery Disease-Reply.JAMA Intern Med. 2020 Jan 1;180(1):166-167. doi: 10.1001/jamainternmed.2019.5857. JAMA Intern Med. 2020. PMID: 31904792 No abstract available.
References
-
- Windecker S, Kolh P, Alfonso F, et al. ; Authors/Task Force Members . 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541-2619. doi: 10.1093/eurheartj/ehu278 - DOI - PubMed
-
- Shaw LJ, Weintraub WS, Maron DJ, et al. Baseline stress myocardial perfusion imaging results and outcomes in patients with stable ischemic heart disease randomized to optimal medical therapy with or without percutaneous coronary intervention. Am Heart J. 2012;164(2):243-250. doi: 10.1016/j.ahj.2012.05.018 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
