

Adverse Events in Long-term Care Residents Transitioning From Hospital Back to Nursing Home
- PMID: 31329223
- PMCID: PMC6646976
- DOI: 10.1001/jamainternmed.2019.2005
Adverse Events in Long-term Care Residents Transitioning From Hospital Back to Nursing Home
Abstract
Importance: Transition from hospital to nursing home is a high-risk period for adverse events in long-term care (LTC) residents. Adverse events include harms from medical care, including failure to provide appropriate care.
Objective: To report the incidence, type, severity, and preventability of adverse events in LTC residents transitioning from hospital back to the same LTC facility.
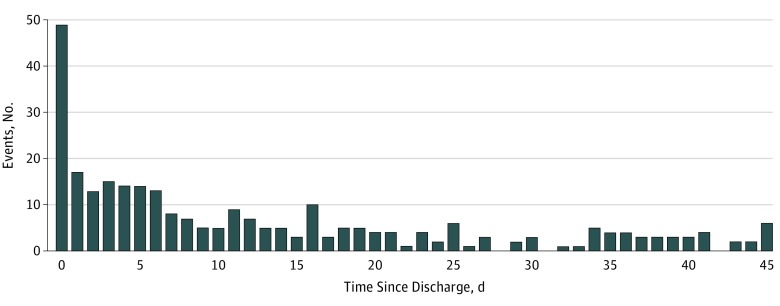
Design, setting, and participants: Prospective cohort study of LTC residents discharged from hospital back to LTC from March 1, 2016, to December 31, 2017, and followed up for 45 days. In a random sample of 32 nursing homes located in 6 New England states, 555 LTC residents were selected, contributing 762 transitions from hospital back to the same LTC facility.
Main outcomes and measures: The main outcome was an adverse event within the 45-day period after transition from hospital back to nursing home. Trained nurse abstractors reviewed nursing home records for the period, and then 2 physicians independently reviewed each potential adverse event to determine whether harm occurred and to characterize the type, severity, and preventability of each event. When reviewers disagreed, they met to reach consensus.
Results: Of the 555 individual residents, 365 (65.6%) were female, and the mean (SD) age at the time of discharge was 82.2 (11.5) years. Five hundred twenty (93.7%) were non-Hispanic white, 21 (3.8%) were non-Hispanic black, 9 (1.6%) were Hispanic, and 5 (0.9%) were of other non-Hispanic race/ethnicity. In the cohort, there were 379 adverse events among 762 discharges. One hundred ninety-seven events (52.0%) related to resident care, with pressure ulcers, skin tears, and falls with injury representing the most common types of events in this category. Health care-acquired infections (108 [28.5%]) and adverse drug events (64 [16.9%]) were the next most common. One hundred ninety-eight (52.2%) adverse events were characterized as less serious. However, 145 (38.3%) events were deemed serious, 28 (7.4%) life-threatening, and 8 (2.1%) fatal. In terms of preventability, 267 (70.4%) adverse events were found to be preventable or ameliorable, with less serious events more often considered preventable or ameliorable (146 [73.7%]) compared with more severe events (121 [66.9%]). In addition, resident care-related adverse events such as fall with injury, skin tear, and pressure ulcer were more commonly deemed preventable (173 of 197 [87.8%]) compared with adverse drug events (39 of 64 [60.9%]) or health care-acquired infections (49 of 108 [45.4%]).
Conclusions and relevance: Adverse events developed in nearly 4 of 10 of discharges from hospital back to LTC. Most were preventable or ameliorable. Standardized reporting of events and better coordination and information transfer across settings are potential ways to prevent adverse events in LTC residents.
Conflict of interest statement
Figures
References
-
- Levinson DR. Adverse Events in Skilled Nursing Facilities: National Incidence Among Medicare Beneficiaries. Washington, DC: Office of Inspector General, Dept of Health & Human Services; 2014.
-
- New England Quality Innovation Network–Quality Improvement Organization Nursing home quality. https://healthcarefornewengland.org/initiatives/nhquality/. Accessed December 22, 2018.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
