

ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer
- PMID: 31329516
- PMCID: PMC6839905
- DOI: 10.1200/JCO.19.00799
ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer
Abstract
Purpose: Enzalutamide, a potent androgen-receptor inhibitor, has demonstrated significant benefits in metastatic and nonmetastatic castration-resistant prostate cancer. We evaluated the efficacy and safety of enzalutamide in metastatic hormone-sensitive prostate cancer (mHSPC).
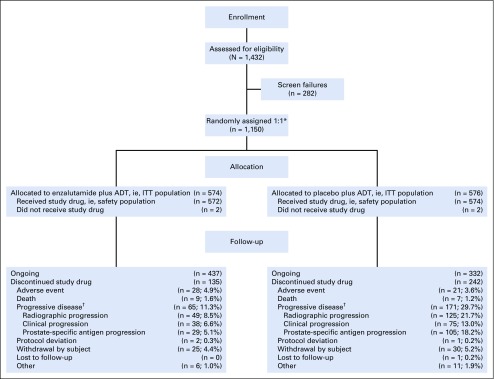
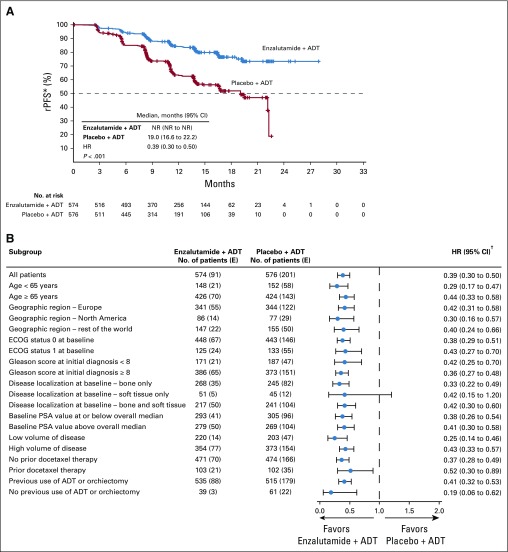
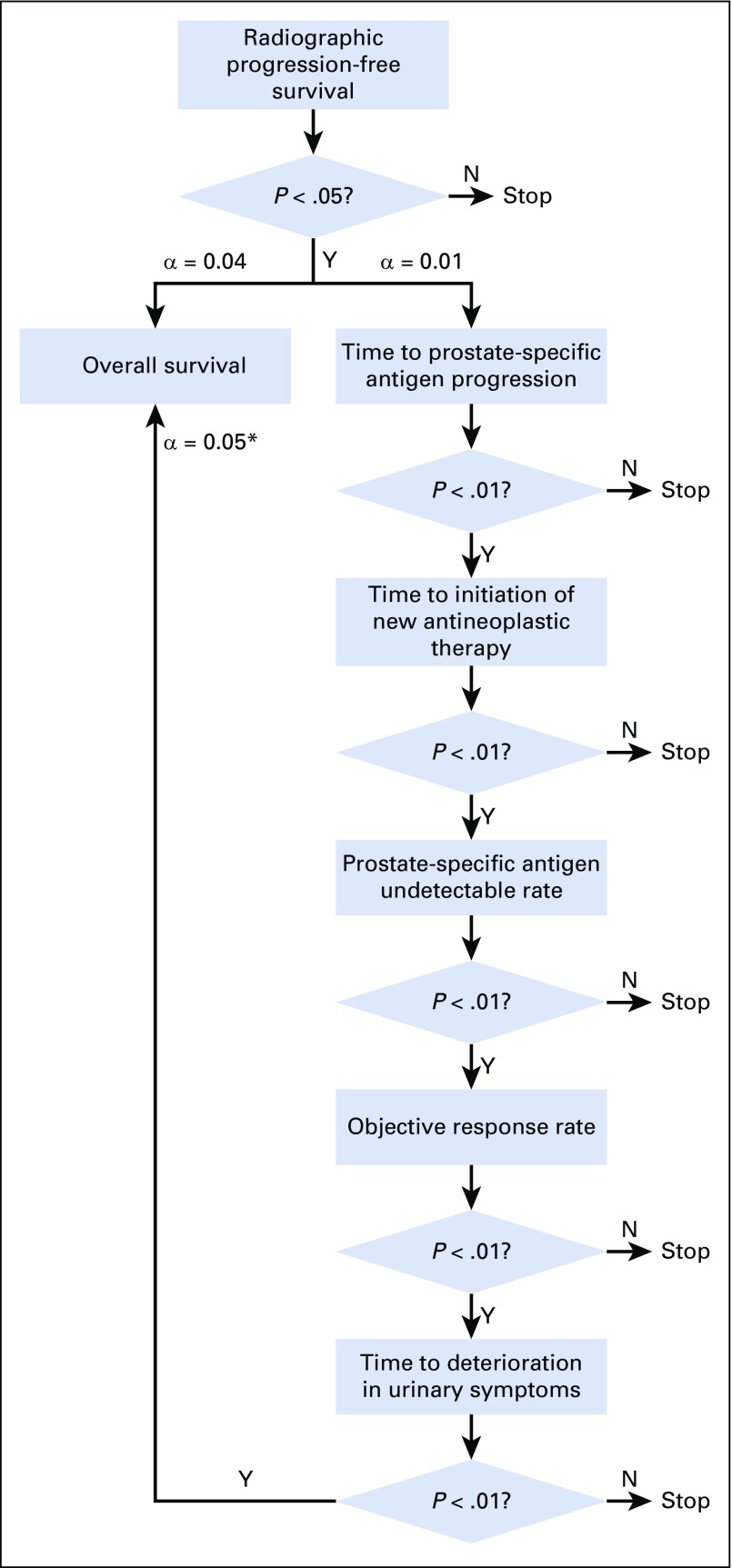
Methods: ARCHES (ClinicalTrials.gov identifier: NCT02677896) is a multinational, double-blind, phase III trial, wherein 1,150 men with mHSPC were randomly assigned 1:1 to enzalutamide (160 mg/day) or placebo, plus androgen deprivation therapy (ADT), stratified by disease volume and prior docetaxel chemotherapy. The primary end point was radiographic progression-free survival.
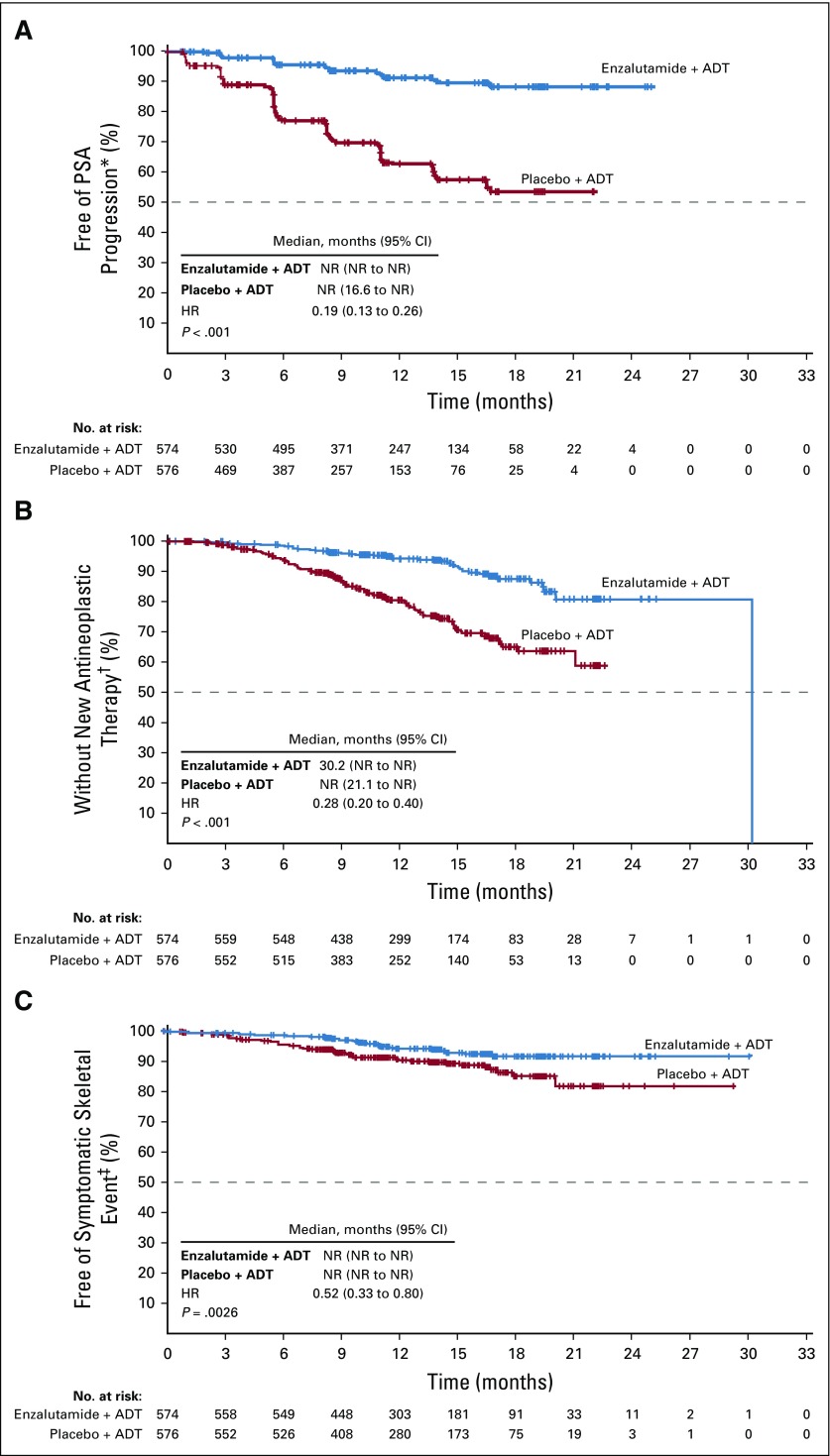
Results: As of October 14, 2018, the risk of radiographic progression or death was significantly reduced with enzalutamide plus ADT versus placebo plus ADT (hazard ratio, 0.39; 95% CI, 0.30 to 0.50; P < .001; median not reached v 19.0 months). Similar significant improvements in radiographic progression-free survival were reported in prespecified subgroups on the basis of disease volume and prior docetaxel therapy. Enzalutamide plus ADT significantly reduced the risk of prostate-specific antigen progression, initiation of new antineoplastic therapy, first symptomatic skeletal event, castration resistance, and reduced risk of pain progression. More men achieved an undetectable prostate-specific antigen level and/or an objective response with enzalutamide plus ADT (P < .001). Patients in both treatment groups reported a high baseline level of quality of life, which was maintained over time. Grade 3 or greater adverse events were reported in 24.3% of patients who received enzalutamide plus ADT versus 25.6% of patients who received placebo plus ADT, with no unexpected adverse events.
Conclusion: Enzalutamide with ADT significantly reduced the risk of metastatic progression or death over time versus placebo plus ADT in men with mHSPC, including those with low-volume disease and/or prior docetaxel, with a safety analysis that seems consistent with the safety profile of enzalutamide in previous clinical trials in castration-resistant prostate cancer.
Figures
Comment in
-
Progress in the Systemic Management of Advanced Prostate Cancer: The Hormone-Sensitive Paradigm.J Clin Oncol. 2019 Nov 10;37(32):2957-2960. doi: 10.1200/JCO.19.01863. Epub 2019 Sep 4. J Clin Oncol. 2019. PMID: 31483709 No abstract available.
References
-
- Fitzmaurice C, Akinyemiju TF, Al Lami FH, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the global burden of disease study. JAMA Oncol. 2018;4:1553–1568. - PMC - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Helgstrand JT, Røder MA, Klemann N, et al. Diagnostic characteristics of lethal prostate cancer. Eur J Cancer. 2017;84:18–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
