

The utility of magnetic resonance imaging for noninvasive evaluation of diabetic nephropathy
- PMID: 31329940
- PMCID: PMC7282829
- DOI: 10.1093/ndt/gfz066
The utility of magnetic resonance imaging for noninvasive evaluation of diabetic nephropathy
Abstract
Background: Noninvasive quantitative measurement of fibrosis in chronic kidney disease (CKD) would be desirable diagnostically and therapeutically but standard radiologic imaging is too variable for clinical usage. By applying a vibratory force, tissue shear wave stiffness can be measured by magnetic resonance elastography (MRE) that may correlate with progression of kidney fibrosis. Since decreased kidney perfusion decreases tissue turgor and stiffness, we combined newly available three-dimensional MRE shear stiffness measurements with MR arterial spin labeling (ASL) kidney blood flow rates to evaluate fibrosis in diabetic nephropathy.
Methods: Thirty individuals with diabetes and Stage 0-5 CKD and 13 control individuals without CKD underwent noncontrast MRE with concurrent ASL blood flow measurements.
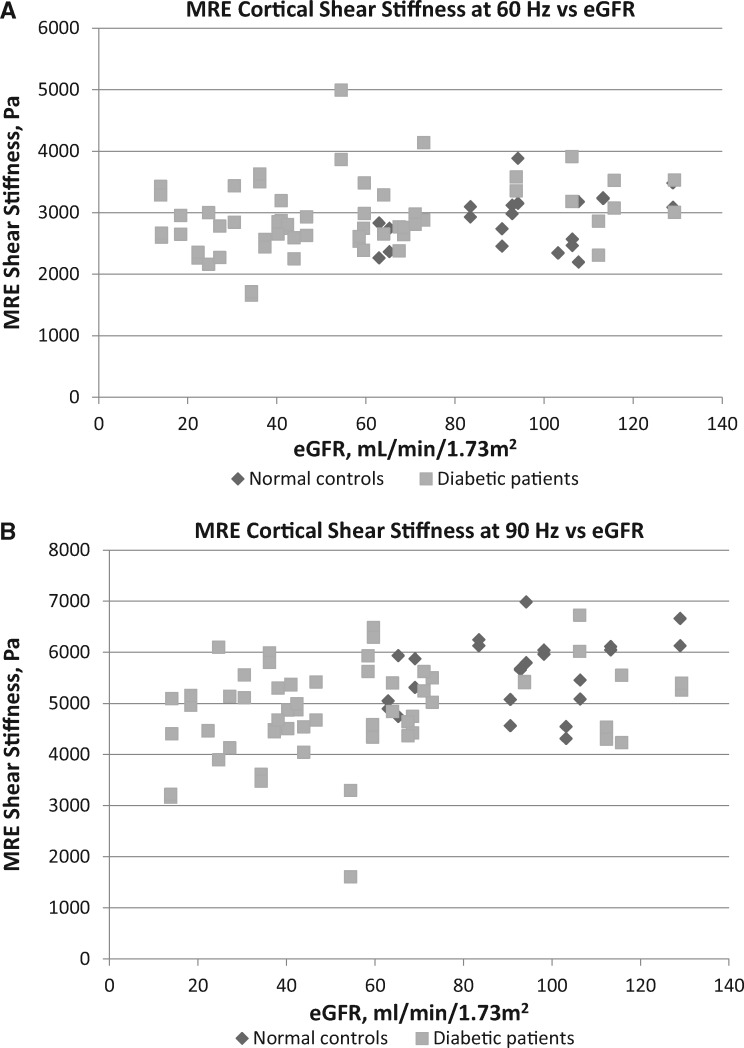
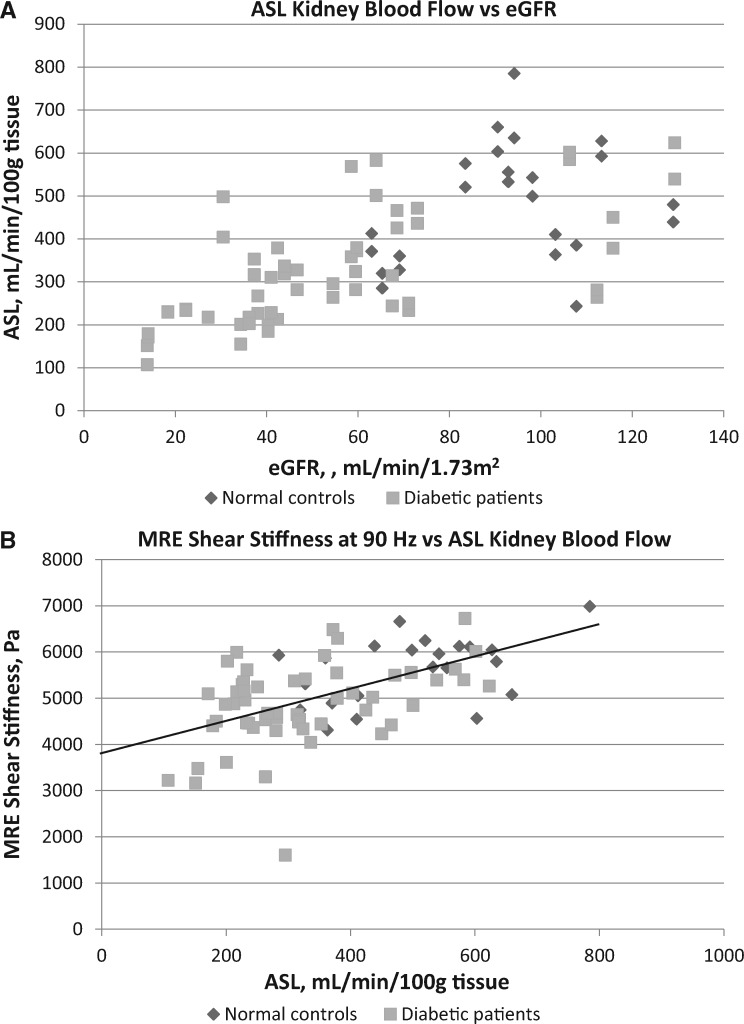
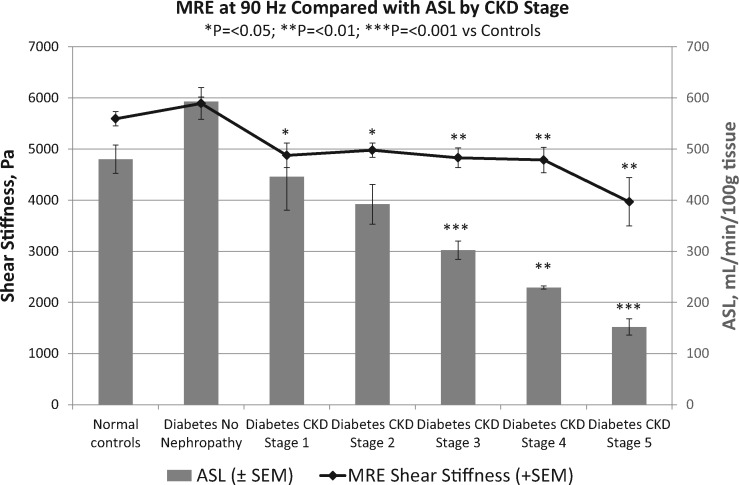
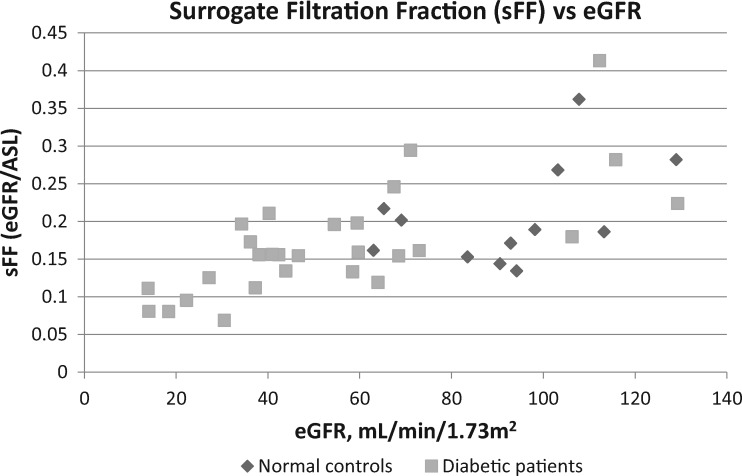
Results: MRE cortical shear stiffness at 90 Hz was decreased significantly below controls in all CKD stages of diabetic nephropathy. Likewise, ASL blood flow decreased progressively from 480 ± 136 mL/min/100 g of cortical tissue in controls to 302 ± 95, 229 ± 7 and 152 ± 32 mL/min/100 g in Stages 3, 4 and 5 CKD, respectively. A magnetic resonance imaging (MRI) surrogate for the measured glomerular filtration fraction [surrogate filtration fraction = estimated glomerular filtration rate (eGFR)/ASL] decreased progressively from 0.21 ± 0.07 in controls to 0.16 ± 0.04 in Stage 3 and 0.10 ± 0.02 in Stage 4-5 CKD.
Conclusions: In this pilot study, MRI with ASL blood flow rates can noninvasively measure decreasing kidney cortical tissue perfusion and, with eGFR, a decreasing surrogate filtration fraction in worsening diabetic nephropathy that appears to correlate with increasing fibrosis. Differing from the liver, MRE shear stiffness surprisingly decreases with worsening CKD, likely related to decreased tissue turgor from lower blood flow rates.
Keywords: chronic kidney disease; diabetic nephropathy; kidney fibrosis; kidney perfusion; magnetic resonance elastography.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Figures
Comment in
-
Recent findings on the clinical utility of renal magnetic resonance imaging biomarkers.Nephrol Dial Transplant. 2020 Jun 1;35(6):915-919. doi: 10.1093/ndt/gfaa125. Nephrol Dial Transplant. 2020. PMID: 32516808 No abstract available.
References
-
- Boor P, Ostendorf T, Floege J.. Renal fibrosis: novel insights into mechanisms and therapeutic targets. Nat Rev Nephrol 2010; 6: 643–656 - PubMed
-
- Rockey DC, Bell PD, Hill JA.. Fibrosis—a common pathway to organ injury and failure. N Engl J Med 2015; 372: 1138–1149 - PubMed
-
- Arndt R, Schmidt S, Loddenkemper C. et al. Noninvasive evaluation of renal allograft fibrosis by transient elastography – a pilot study. Transpl Int 2010; 23: 871–877 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
