

The Molecular Hallmarks of the Serrated Pathway in Colorectal Cancer
- PMID: 31330830
- PMCID: PMC6678087
- DOI: 10.3390/cancers11071017
The Molecular Hallmarks of the Serrated Pathway in Colorectal Cancer
Abstract
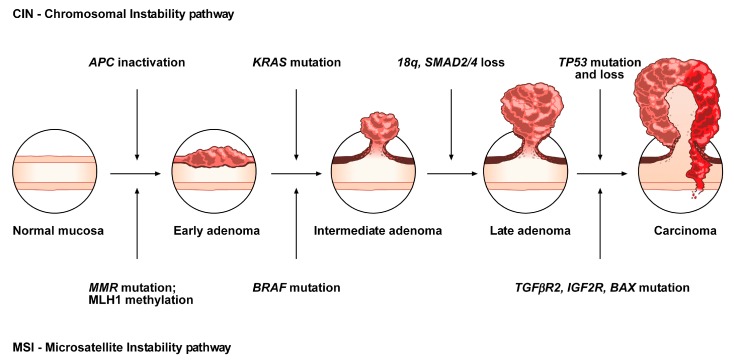
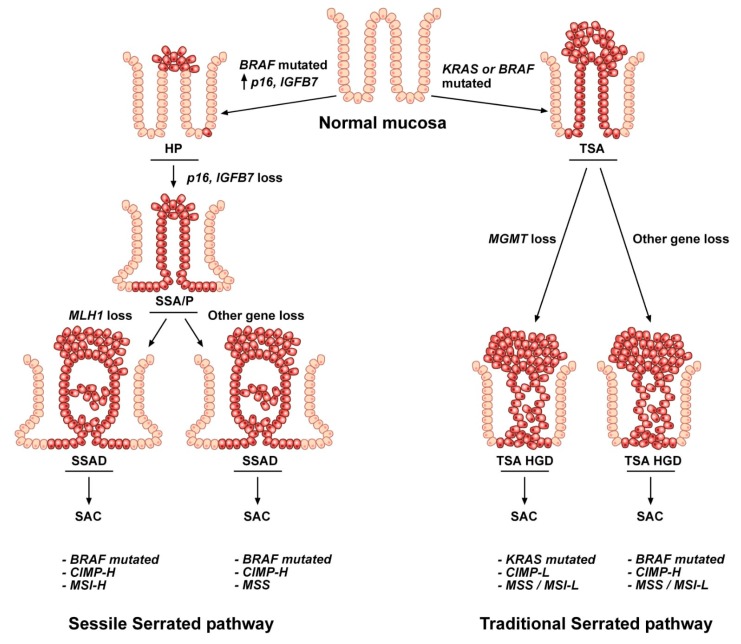
Colorectal cancer (CRC) is a leading cause of cancer death worldwide. It includes different subtypes that differ in their clinical and prognostic features. In the past decade, in addition to the conventional adenoma-carcinoma model, an alternative multistep mechanism of carcinogenesis, namely the "serrated pathway", has been described. Approximately, 15 to 30% of all CRCs arise from neoplastic serrated polyps, a heterogeneous group of lesions that are histologically classified into three morphologic categories: hyperplastic polyps, sessile serrated adenomas/polyps, and the traditional serrated adenomas/polyps. Serrated polyps are characterized by genetic (BRAF or KRAS mutations) and epigenetic (CpG island methylator phenotype (CIMP)) alterations that cooperate to initiate and drive malignant transformation from normal colon mucosa to polyps, and then to CRC. The high heterogeneity of the serrated lesions renders their diagnostic and pathological interpretation difficult. Hence, novel genetic and epigenetic biomarkers are required for better classification and management of CRCs. To date, several molecular alterations have been associated with the serrated polyp-CRC sequence. In addition, the gut microbiota is emerging as a contributor to/modulator of the serrated pathway. This review summarizes the state of the art of the genetic, epigenetic and microbiota signatures associated with serrated CRCs, together with their clinical implications.
Keywords: CIMP; CIN; DNA methylation; MSI; colorectal cancer; gut microbiota; serrated adenocarcinoma; serrated lesions; serrated pathway; serrated polyp.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Wong K., Xie G. Updates on the Molecular Genetics of Colorectal Cancer. Colorectal Cancer Open Access. 2017;3 doi: 10.21767/2471-9943.100032. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
