

Surgical anatomy of the ovine sural nerve for facial nerve regeneration and reconstruction research
- PMID: 31332199
- PMCID: PMC6646377
- DOI: 10.1038/s41598-019-46661-3
Surgical anatomy of the ovine sural nerve for facial nerve regeneration and reconstruction research
Abstract
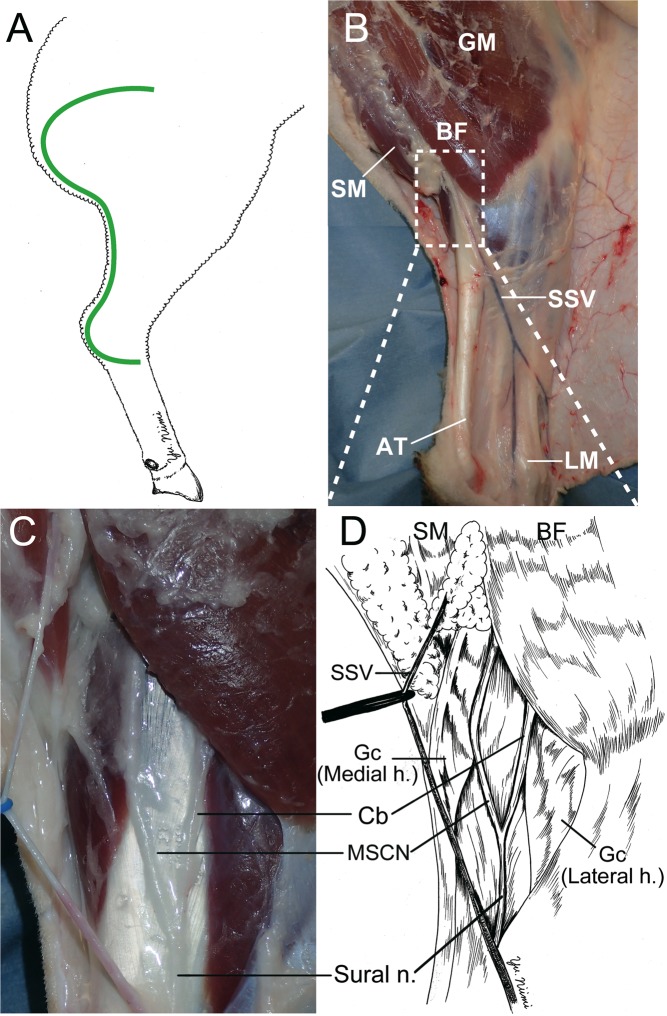
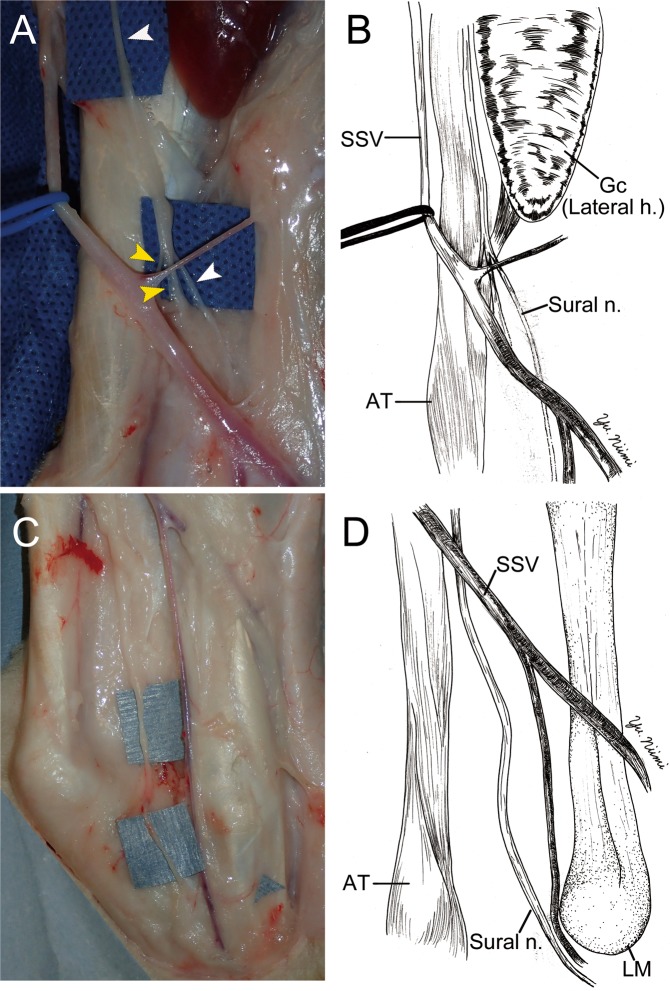
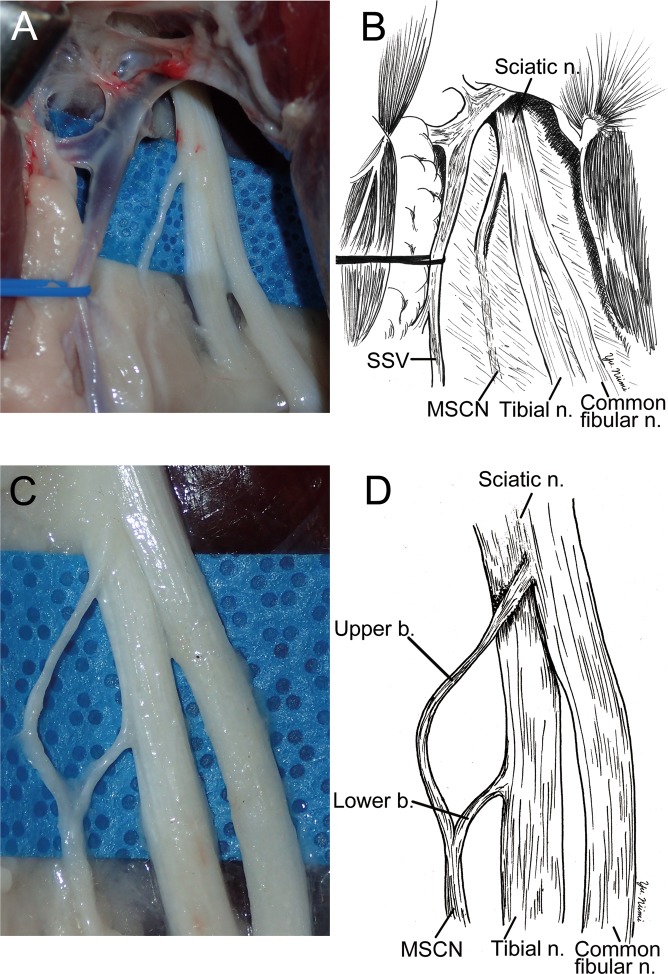
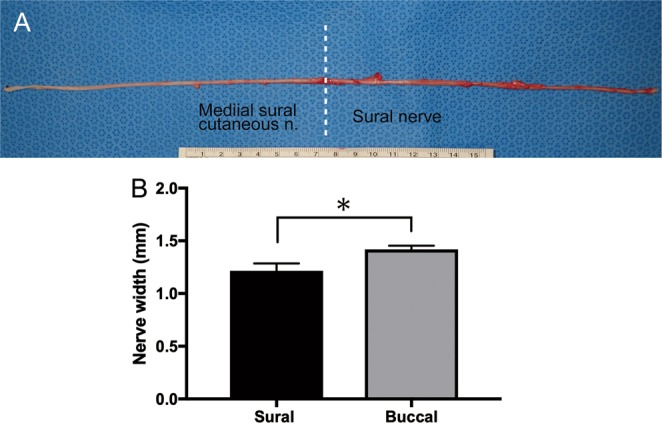
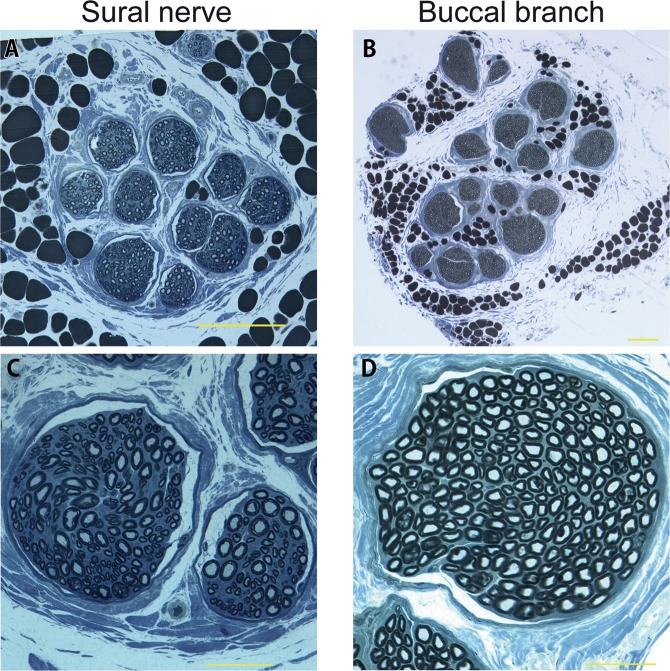
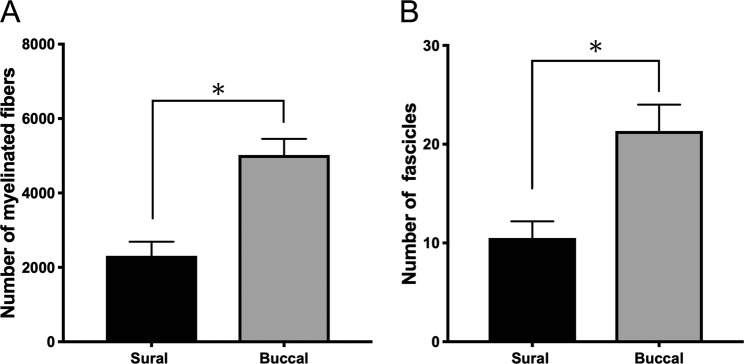
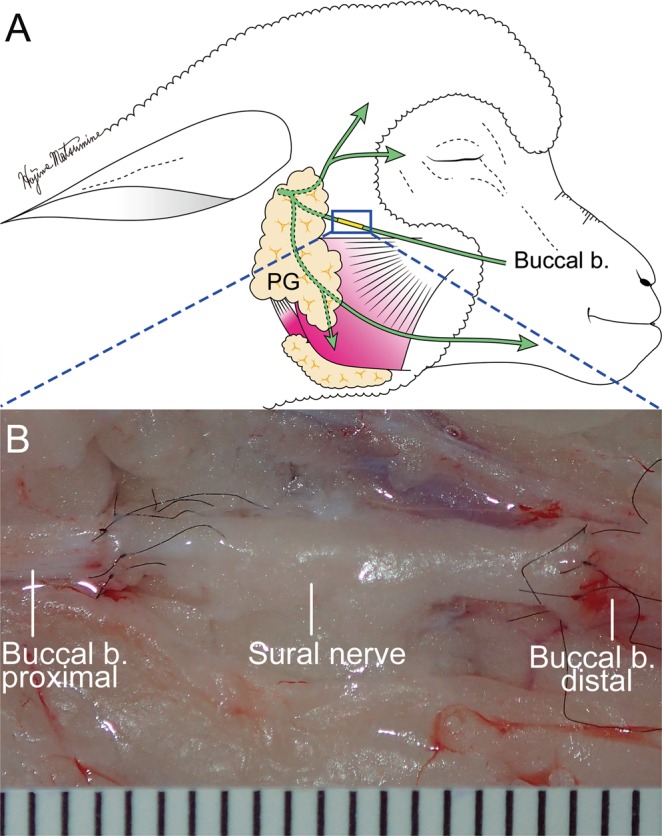
The lack of a clinically relevant animal models for research in facial nerve reconstruction is challenging. In this study, we investigated the surgical anatomy of the ovine sural nerve as a potential candidate for facial nerve reconstruction, and performed its histological quantitative analysis in comparison to the buccal branch (BB) of the facial nerve using cadaver and anesthetized sheep. The ovine sural nerve descended to the lower leg along the short saphenous vein. The length of the sural nerve was 14.3 ± 0.5 cm. The distance from the posterior edge of the lateral malleolus to the sural nerve was 7.8 ± 1.8 mm. The mean number of myelinated fibers in the sural nerve was significantly lower than that of the BB (2,311 ± 381vs. 5,022 ± 433, respectively. p = 0.003). The number of fascicles in the sural nerve was also significantly lower than in the BB (10.5 ± 1.7 vs. 21.3 ± 2.7, respectively. p = 0.007). The sural nerve was grafted to the BB with end-to-end neurorrhaphy under surgical microscopy in cadaver sheep. The surgical anatomy and the number of fascicles of the ovine sural nerve were similar of those reported in humans. The results suggest that the sural nerve can be successfully used for facial nerve reconstruction research in a clinically relevant ovine model.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
