

Mapping exclusive breastfeeding in Africa between 2000 and 2017
- PMID: 31332393
- PMCID: PMC6749549
- DOI: 10.1038/s41591-019-0525-0
Mapping exclusive breastfeeding in Africa between 2000 and 2017
Erratum in
-
Publisher Correction: Mapping exclusive breastfeeding in Africa between 2000 and 2017.Nat Med. 2019 Sep;25(9):1458. doi: 10.1038/s41591-019-0577-1. Nat Med. 2019. PMID: 31455921 Free PMC article.
Abstract
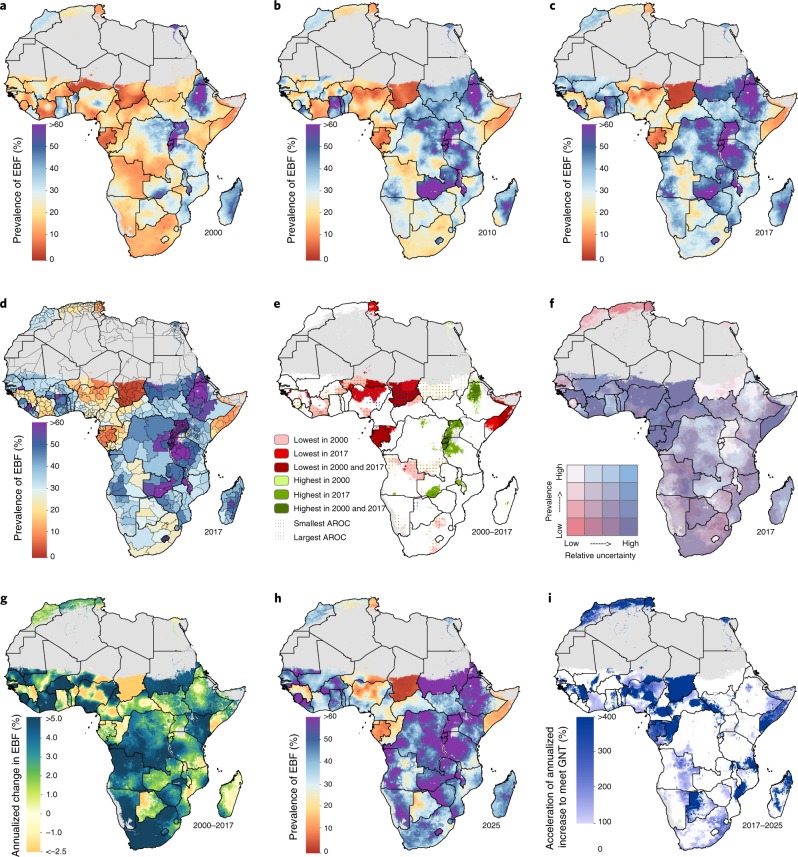
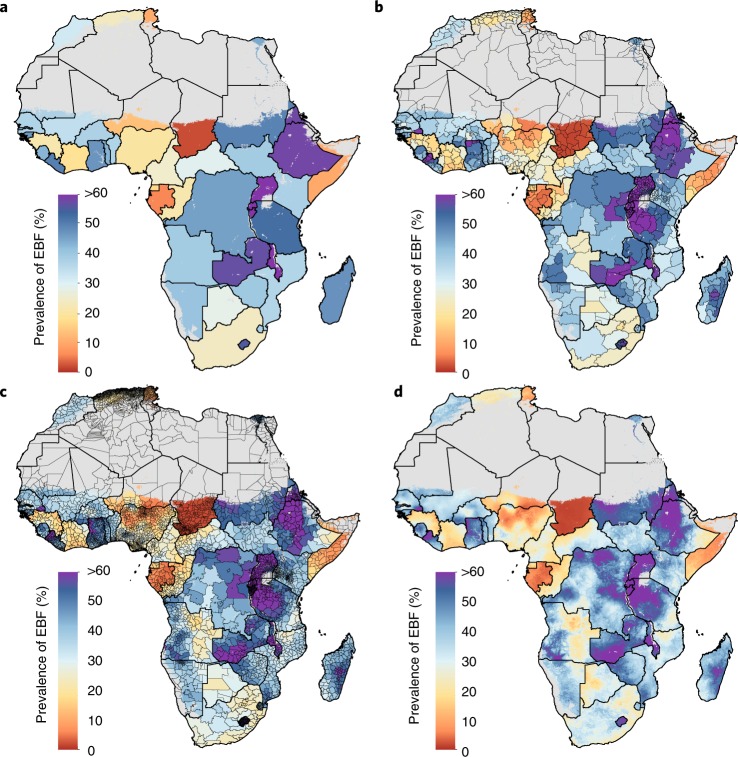
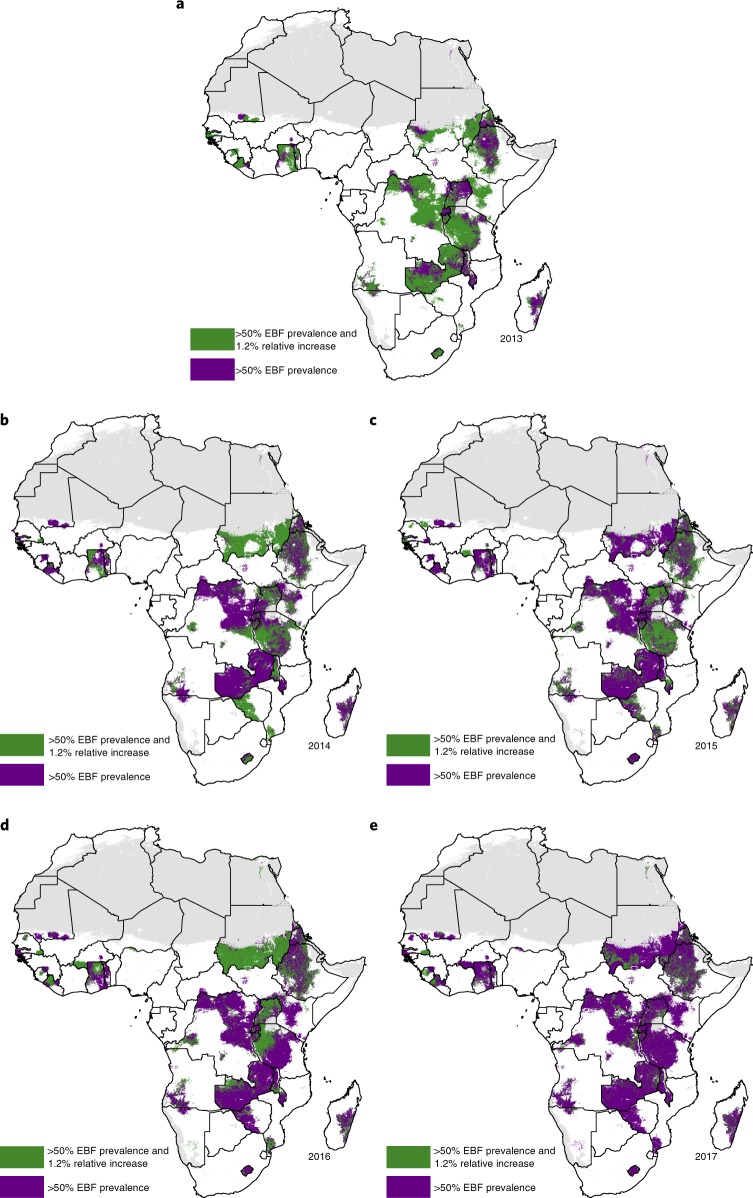
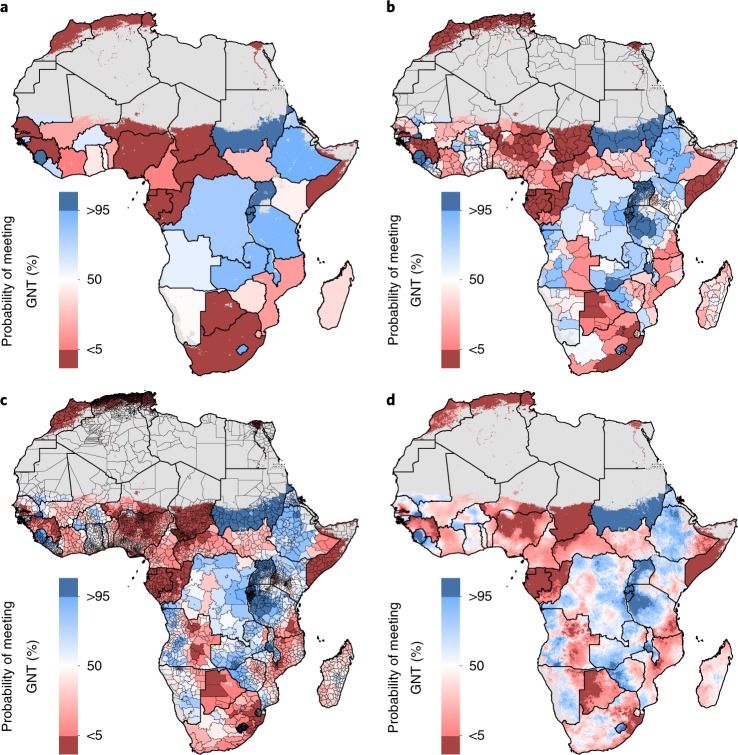
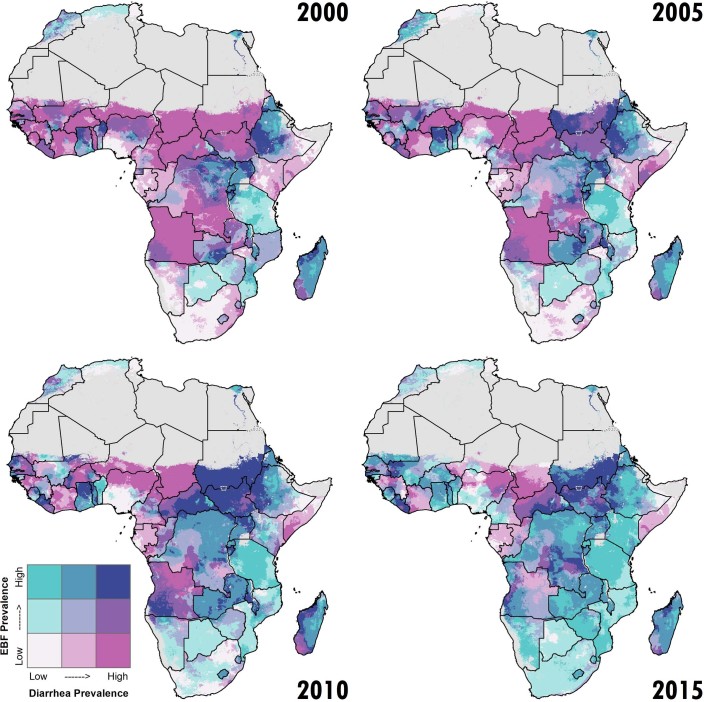
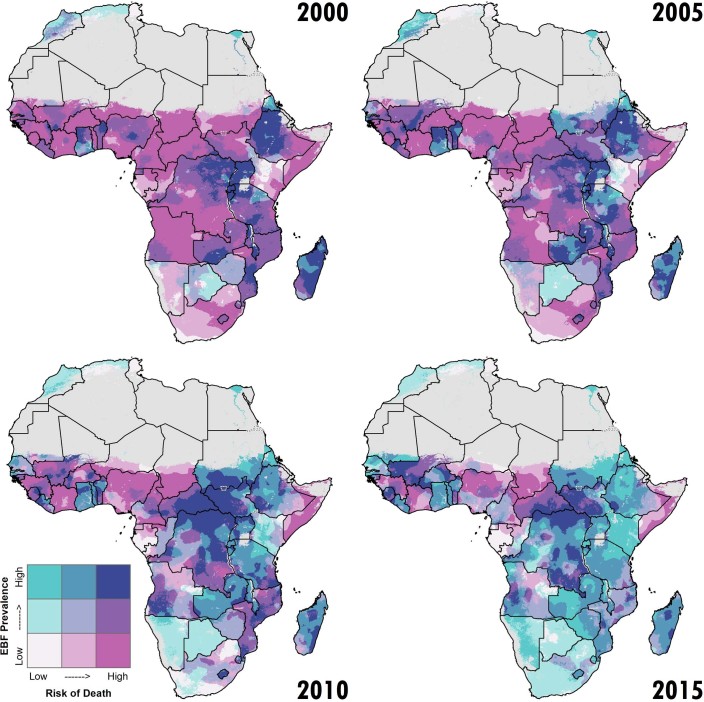
Exclusive breastfeeding (EBF)-giving infants only breast-milk (and medications, oral rehydration salts and vitamins as needed) with no additional food or drink for their first six months of life-is one of the most effective strategies for preventing child mortality1-4. Despite these advantages, only 37% of infants under 6 months of age in Africa were exclusively breastfed in 20175, and the practice of EBF varies by population. Here, we present a fine-scale geospatial analysis of EBF prevalence and trends in 49 African countries from 2000-2017, providing policy-relevant administrative- and national-level estimates. Previous national-level analyses found that most countries will not meet the World Health Organization's Global Nutrition Target of 50% EBF prevalence by 20256. Our analyses show that even fewer will achieve this ambition in all subnational areas. Our estimates provide the ability to visualize subnational EBF variability and identify populations in need of additional breastfeeding support.
Conflict of interest statement
This study was funded by the Bill & Melinda Gates Foundation. Co-authors employed by the Bill & Melinda Gates Foundation provided feedback on initial maps and drafts of this manuscript. Otherwise, the funders had no role in study design, data collection, data analysis, data interpretation, writing of the final report, or decision to publish. The corresponding author had full access to all of the data in the study, and had final responsibility for the decision to submit for publication.
Figures
References
-
- Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: The Integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD) (WHO & UNICEF, 2013). - PubMed
-
- Stanaway JD, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923–1994. doi: 10.1016/S0140-6736(18)32225-6. - DOI - PMC - PubMed
