

Genicular Nerve Radiofrequency Ablation for Painful Knee Arthritis: The Why and the How
- PMID: 31333900
- PMCID: PMC6635137
- DOI: 10.2106/JBJS.ST.18.00016
Genicular Nerve Radiofrequency Ablation for Painful Knee Arthritis: The Why and the How
Abstract
Background: Genicular nerve radiofrequency ablation (GNRFA), including conventional, cooled, and pulsed techniques, has been used in the management of symptomatic knee osteoarthritis (OA). This new and innovative treatment option has the capacity to decrease pain and improve function and quality of life in certain patients. GNRFA is reserved for patients with symptomatic knee OA who have had failure of conservative treatment and have had failure of or are poor candidates for surgery. GNRFA has been shown to consistently provide short-term (3 to 6-month), and sometimes longer, pain relief in patients. GNRFA has been demonstrated to be safe to administer repeatedly in patients who respond well to this minimally invasive procedure.
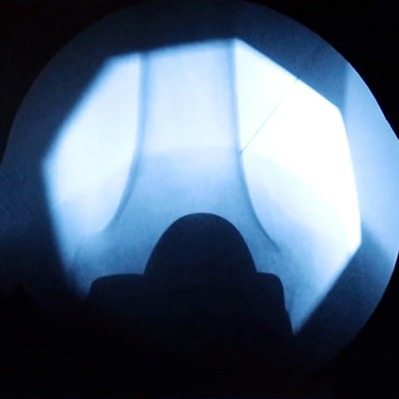
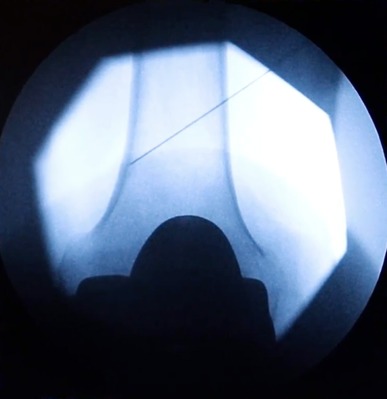
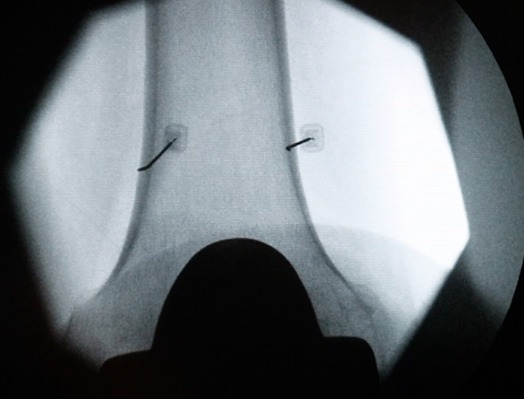
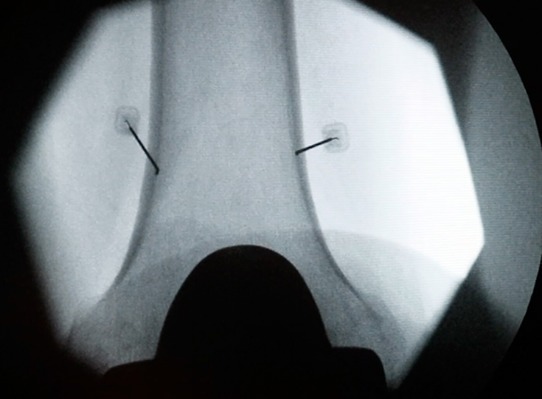
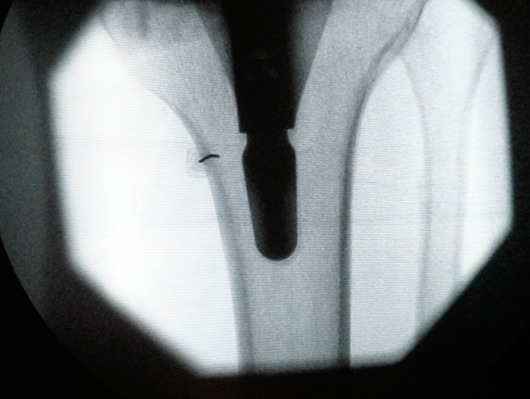
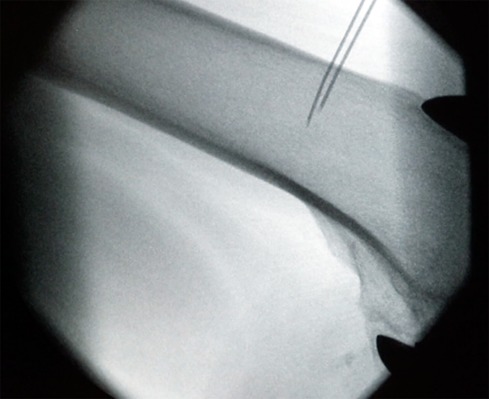
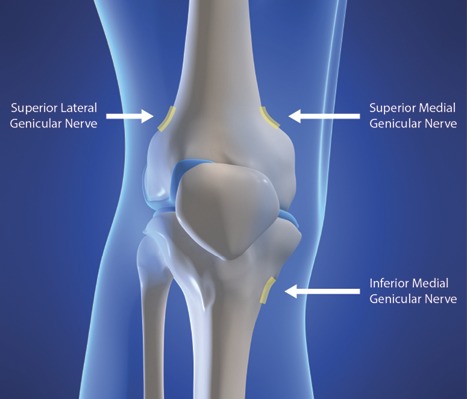
Description: GNRFA is a 2-step procedure. First, patients are given a diagnostic block under fluoroscopy or ultrasound guidance. Specifically, 1 mL of lidocaine is injected using a 20-gauge, 3.5-in (8.9-cm) spinal needle around the superior lateral, superior medial, and inferior medial genicular nerve branches. The diagnostic block is extra-articular. If the patient reports a ≥50% reduction in baseline pain for a minimum of 24 hours following the injection, then the patient is a candidate for genicular ablation. The osseous landmarks for the diagnostic block are exactly the same as for the ablation procedure. Both procedures are well tolerated in the office setting under local skin anesthesia or can be done in the operating room under conscious sedation using a low-dose sedative such as midazolam for anxious patients. General anesthesia is not required for GNRFA. This procedure is most commonly performed by interventional pain specialists but may also be performed by any physician with appropriate training. In some jurisdictions, physician assistants and nurse practitioners may perform this procedure subject to their supervision requirements.
Alternatives: Conservative treatment for symptomatic knee OA includes weight loss management, physical and aquatic therapy, bracing, lateral wedge insoles, transcutaneous nerve stimulation, nonsteroidal anti-inflammatory drugs in combination with a proton pump inhibitor, autologous blood-based therapies, and cortisone and hyaluronic acid injections1,2. Surgical treatment for symptomatic knee OA includes knee arthroscopy, high tibial osteotomy, total knee replacement, and unicompartmental knee replacement in patients without lateral compartment disease2. It should be noted that there is some evidence suggesting that steroid injection, viscosupplements, and arthroscopy are not effective for the management of knee OA.
Rationale: Thermal GNRFA differs from all other treatment alternatives because this procedure causes denaturing of the 3 sensory nerves primarily responsible for transmitting knee pain from an arthritic joint to the central nervous system. In this procedure, heating occurs from an intense alternating electrical field at the tip of the cannula, which produces sufficient heat to denature the proteins in the target tissue. The accepted heating parameters for this procedure are 70° to 80°C for 60 or 90 seconds. A commonly raised question is whether this procedure precipitates a Charcot-type joint. The Charcot joint involves much more than reduced innervation; it occurs in the context of chronically compromised vascularity and altered soft-tissue characteristics as well as peripheral neuropathy. Moreover, a Charcot-type joint does not develop because the deafferentation of the weight-bearing joint is partial3. To our knowledge, no Charcot-type joints have been reported after this procedure. Conversely, data from an animal study have shown that selective joint denervation may lead to the progression of knee OA4. The ablation procedure is done outside the knee joint, unlike alternatives such as intra-articular therapies and surgery. The effectiveness of nonsurgical knee OA interventions in alleviating pain and improving joint function is generally inadequate1. However, GNRFA appears to be an emerging alternative for patients who have had failure of conservative and surgical treatments. It is not uncommon in our clinical practice for patients to achieve adequate pain control following ablation for up to 1 year. GNRFA provides temporary relief from symptomatic knee OA because it does not eliminate the potential for peripheral nerve regrowth and regeneration, and thus pain, to return.
Figures


Similar articles
-
Genicular nerve radiofrequency ablation practice patterns: A survey study of the International Pain and Spine Interventional Society.Interv Pain Med. 2024 Aug 19;3(3):100432. doi: 10.1016/j.inpm.2024.100432. eCollection 2024 Sep. Interv Pain Med. 2024. PMID: 39502912 Free PMC article.
-
Comparing effectiveness of 3-needle approach versus 5-needle approach of genicular nerve block on pain and quality of life in chronic osteoarthritis of knee: a double blinded randomised controlled trial.BMC Musculoskelet Disord. 2024 Nov 29;25(1):978. doi: 10.1186/s12891-024-07938-5. BMC Musculoskelet Disord. 2024. PMID: 39614201 Free PMC article. Clinical Trial.
-
Comparison of Radiation Exposure Between Trident and Conventional Cannula in Genicular RF Procedures Under Fluoroscopy for Gonarthrosis.Pain Physician. 2025 May;28(3):E233-E242. Pain Physician. 2025. PMID: 40464891
-
Safety and Efficacy of Genicular Nerve Radiofrequency Ablation for Management of Painful Total Knee Replacement: A Systematic Review.Cureus. 2021 Nov 11;13(11):e19489. doi: 10.7759/cureus.19489. eCollection 2021 Nov. Cureus. 2021. PMID: 34912630 Free PMC article. Review.
-
The Analgesic Effectiveness of Genicular Nerve-targeted Cooled and Pulsed Radiofrequency Ablation for Osteoarthritis Knee Pain: A Systematic Review and Meta-analysis.Pain Physician. 2024 Sep;27(7):357-373. Pain Physician. 2024. PMID: 39353105
Cited by
-
Review of genicular artery embolization, radiofrequency ablation, and cryoneurolysis in the management of osteoarthritis-related knee pain.Diagn Interv Radiol. 2023 Jul 20;29(4):614-620. doi: 10.4274/dir.2022.221288. Epub 2023 Jan 9. Diagn Interv Radiol. 2023. PMID: 36960623 Free PMC article.
-
Genicular nerve radiofrequency ablation for pain control following anterior cruciate ligament reconstruction - A case report.Trauma Case Rep. 2022 May 24;40:100661. doi: 10.1016/j.tcr.2022.100661. eCollection 2022 Aug. Trauma Case Rep. 2022. PMID: 35665197 Free PMC article.
-
Effectiveness comparison of genicular nerve ablation for knee osteoarthritic versus post-total knee arthroplasty pain.Interv Pain Med. 2024 Feb 24;3(1):100390. doi: 10.1016/j.inpm.2024.100390. eCollection 2024 Mar. Interv Pain Med. 2024. PMID: 39239503 Free PMC article.
-
Interventional Techniques for the Management of Knee Osteoarthritis: A Literature Review.Cureus. 2023 Oct 16;15(10):e47133. doi: 10.7759/cureus.47133. eCollection 2023 Oct. Cureus. 2023. PMID: 38022320 Free PMC article. Review.
-
Radiofrequency Ablation for the Knee Joint: A Survey by the American Society of Pain and Neuroscience.J Pain Res. 2022 Apr 27;15:1247-1255. doi: 10.2147/JPR.S342653. eCollection 2022. J Pain Res. 2022. PMID: 35509622 Free PMC article.
References
-
- Dellon AL. Partial knee joint denervation for the knee pain: a review. Orthop Muscul Syst. 2014;3:167.
-
- Salo PT, Hogervorst T, Seerattan RA, Rucker D, Bray RC. Selective joint denervation promotes knee osteoarthritis in the aging rat. J Orthop Res. 2002. November;20(6):1256-64. - PubMed