

An Update on Measures of Preoperative Glycemic Control
- PMID: 31333965
- PMCID: PMC6571350
- DOI: 10.1097/GOX.0000000000002240
An Update on Measures of Preoperative Glycemic Control
Abstract
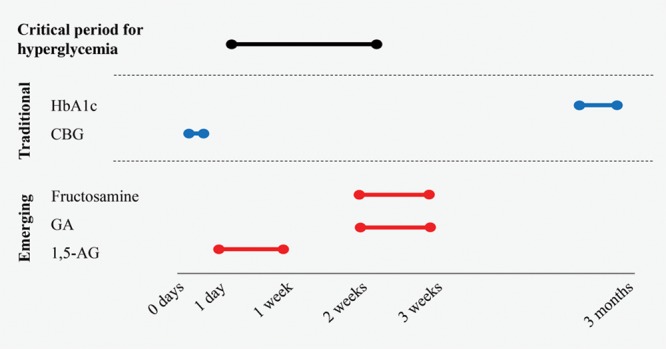
Glycemic control represents a modifiable preoperative risk factor in surgery. Traditionally, hemoglobin A1c (HbA1c) and plasma glucose are utilized as measures of glycemic control. However, studies show mixed results regarding the ability of these conventional measures to predict adverse surgical outcomes. This may be explained by the time window captured by HbA1c and serum glucose: long-term and immediate glycemic control, respectively. Fructosamine, glycosylated albumin, and 1,5-anhydroglucitol constitute alternative metrics of glycemic control that are of growing interest but are underutilized in the field of surgery. These nontraditional measures reflect the temporal variations in glycemia over the preceding days to weeks. Therefore, they may more accurately reflect glycemic control within the time window that most significantly affects surgical outcomes. Additionally, these alternative measures are predictive of negative outcomes, even in the nondiabetic population and in patients with chronic renal disease and anemia, for whom HbA1c performs poorly. Adopting these newer metrics of glycemia may enhance the value of preoperative evaluation, such that the effectiveness of any preoperative glycemic control interventions can be assessed, and adverse outcomes associated with hyperglycemia better predicted. The goal of this review is to provide an update on the preoperative management of glycemia and to describe alternative metrics that may improve our ability to predict and control for the negative outcomes associated with poor glycemic control.
Figures
References
-
- Ibrahim AM, Shuster M, Koolen PG, et al. Analysis of the National Surgical Quality Improvement Program database in 19,100 patients undergoing implant-based breast reconstruction: complication rates with acellular dermal matrix. Plast Reconstr Surg. 2013;132:1057–1066. - PubMed
-
- Bamba R, Gupta V, Shack RB, et al. Evaluation of diabetes mellitus as a risk factor for major complications in patients undergoing aesthetic surgery. Aesthet Surg J. 2016;36:598–608. - PubMed
-
- Dortch JD, Eck DL, Ladlie B, et al. Perioperative glycemic control in plastic surgery: review and discussion of an institutional protocol. Aesthet Surg J. 2016;36:821–830. - PubMed
-
- Golden SH, Peart-Vigilance C, Kao WH, et al. Perioperative glycemic control and the risk of infectious complications in a cohort of adults with diabetes. Diabetes Care. 1999;22:1408–1414. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical