

Congenital Pseudarthrosis of the Tibia: Results, at Skeletal Maturity, of the Charnley-Williams Procedure
- PMID: 31334459
- PMCID: PMC6613849
- DOI: 10.2106/JBJS.OA.19.00004
Congenital Pseudarthrosis of the Tibia: Results, at Skeletal Maturity, of the Charnley-Williams Procedure
Abstract
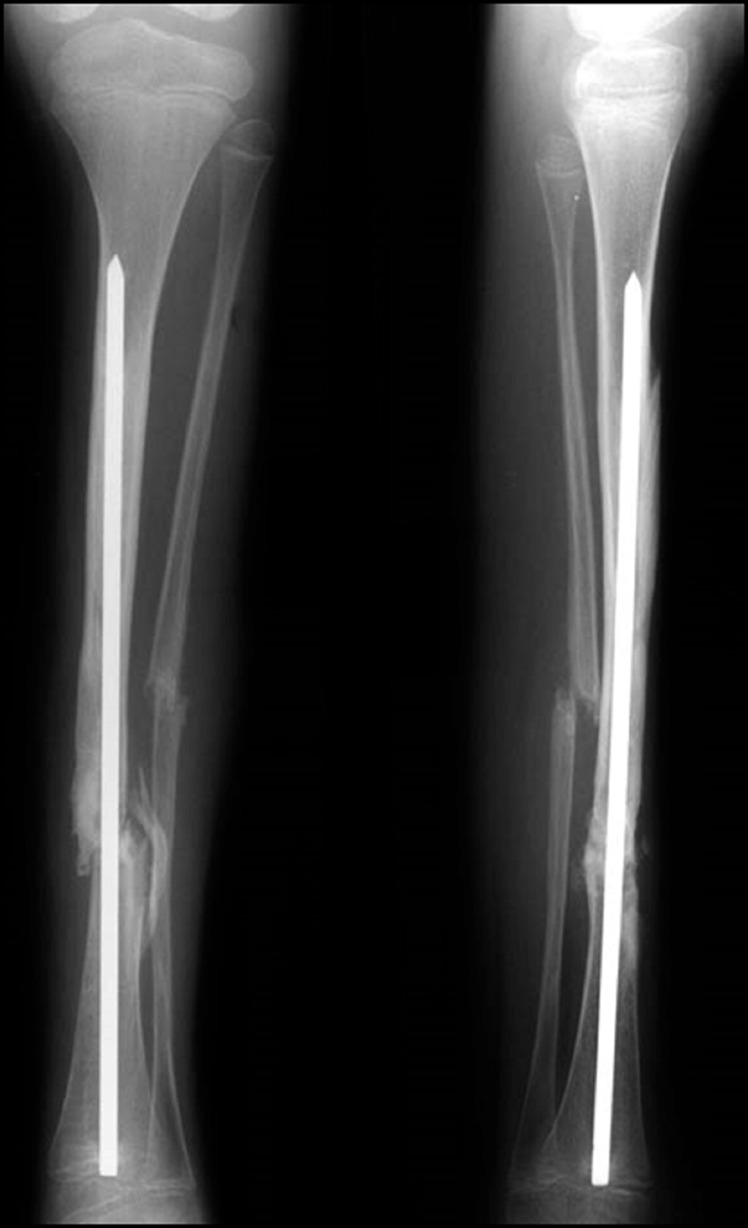
Background: This study assessed the outcomes, at skeletal maturity, for 34 patients in whom congenital pseudarthrosis of the tibia (CPT) had been treated with intramedullary (IM) rod fixation.
Methods: The results in skeletally mature patients in whom type-4 CPT had been treated with an IM rod at an average of 11.9 years earlier were reviewed. The rod procedures varied according to whether both the tibia and the fibula were resected and both bones (type A) or just the tibia (type B) were fixed with an IM rod or whether only the tibia was resected and the fibula received no surgery (type C). Outcome grading ranged from unequivocal union with brace-free function (grade 1) to a functional limb with residual angulation or cortical defects (grade 2) to a severely impaired extremity with insufficient union or refracture (grade 3).
Results: Thirty-four patients were evaluated at a mean age of 16.9 years, a mean of 11.9 years after their initial surgical procedure. Seventeen patients had a grade-1 result; 11 patients, grade 2; and 6, grade 3. Thus, 82% (28) of the 34 patients had a functional extremity at maturity. All patients with a final grade-3 outcome eventually requested amputation. The final outcomes were not affected by the age at the initial fracture or surgery, the presence of neurofibromatosis-1, or cross-ankle fixation. A total of 58 IM rod procedures were performed in the 34 patients. Twenty-four (73%) of the 33 type-A procedures produced grade-1 or 2 outcomes, as did 14 (88%) of the 16 type-B procedures. Of the 9 type-C procedures, none produced a grade-1 result and 4 produced a grade-2 outcome. The results of types A and B combined were superior to those of type-C procedures (p = 0.03). Refracture occurred in 13 of 33 patients with initial stability/union after rod fixation, with 3 of those fractures remaining ununited at the latest follow-up. A dystrophic fibula had no effect on the eventual achievement of a grade-1 or 2 outcome.
Conclusions: This review, in which all patients had reached skeletal maturity, documents functional (grade-1 or 2) outcomes in 82% of cases of IM rod fixation for CPT. This finding was almost identical to the result in our earlier report and confirms the long-term value of permanent IM rod fixation in maintaining union and function in patients with CPT. Procedures not addressing the fibula produced inferior results. Although 13 patients had a refracture following initial union, only 3 of these fractures failed to heal with additional treatment.
Level of evidence: Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
Figures


References
-
- Charnley J. Congenital pseudarthrosis of the tibia treated by intramedullary nail. J Bone Joint Surg Am. 1956. April;38(2):283-90. - PubMed
-
- Williams PF. Fragmentation and rodding in osteogenesis imperfecta. J Bone Joint Surg Br. 1965. February;47:23-31. - PubMed
-
- Johnston CE., 2nd. Congenital pseudarthrosis of the tibia: results of technical variations in the Charnley-Williams procedure. J Bone Joint Surg Am. 2002. October;84(10):1799-810. - PubMed
-
- Dobbs MB, Rich MM, Gordon JE, Szymanski DA, Schoenecker PL. Use of an intramedullary rod for treatment of congenital pseudarthrosis of the tibia. A long-term follow-up study. J Bone Joint Surg Am. 2004. June;86(6):1186-97. - PubMed
-
- Shah H, Doddabasappa SN, Joseph B. Congenital pseudarthrosis of the tibia treated with intramedullary rodding and cortical bone grafting: a follow-up study at skeletal maturity. J Pediatr Orthop. 2011. Jan-Feb;31(1):79-88. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials