

Posterior Malleolar Ankle Fractures: An Effort at Improving Outcomes
- PMID: 31334465
- PMCID: PMC6613847
- DOI: 10.2106/JBJS.OA.18.00058
Posterior Malleolar Ankle Fractures: An Effort at Improving Outcomes
Abstract
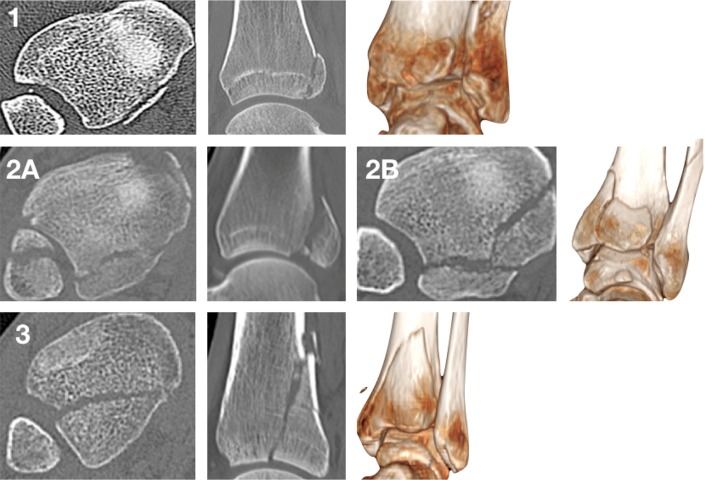
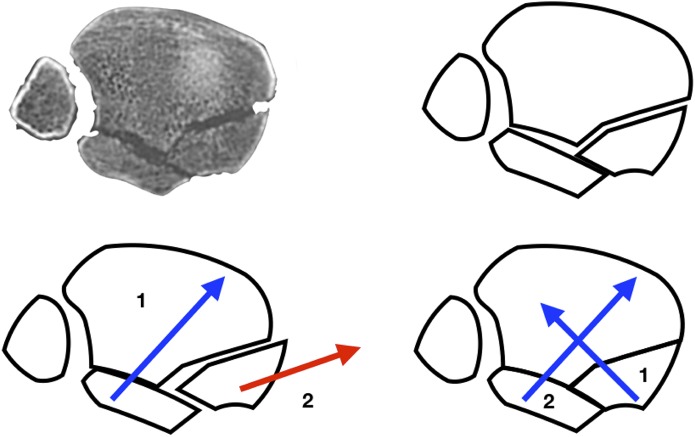
Background: There is increasing acceptance that the clinical outcomes following posterior malleolar fractures are less than satisfactory. We report our results of posterior malleolar fracture management based on the classification by Mason and Molloy.
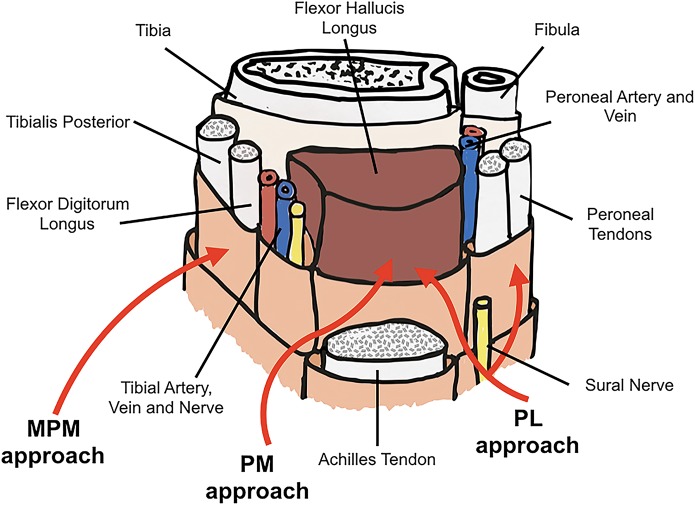
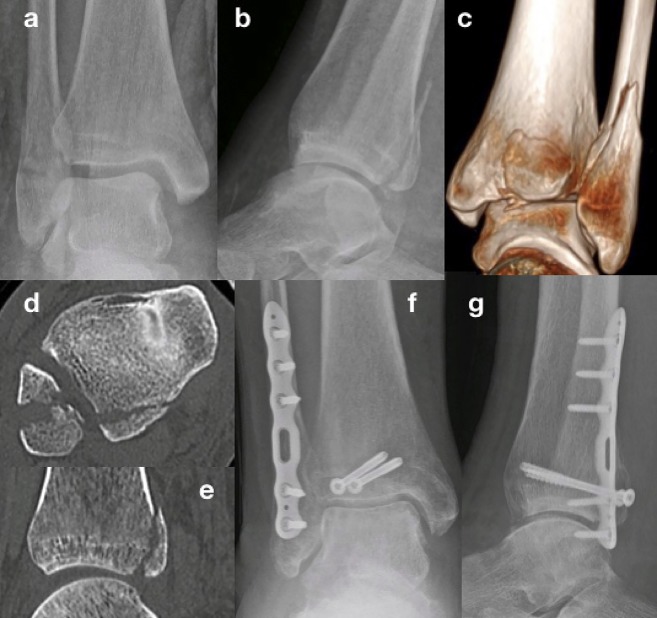
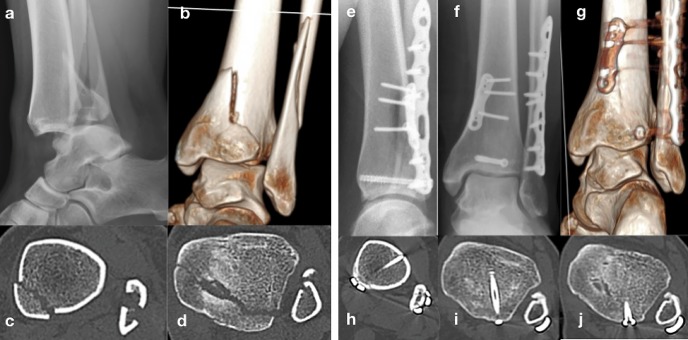
Methods: All fractures were classified on the basis of computed tomographic (CT) scans obtained preoperatively. This dictated the treatment algorithm. Type-1 fractures underwent syndesmotic fixation. Type-2A fractures underwent open reduction and internal fixation through a posterolateral incision, type-2B fractures underwent open reduction and internal fixation through either a posteromedial incision or a combination of a posterolateral with a medial-posteromedial incision, and type-3 fractures underwent open reduction and internal fixation through a posteromedial incision.
Results: Patient-related outcome measures were obtained in 50 patients with at least 1-year follow-up. According to the Mason and Molloy classification, there were 17 type-1 fractures, 12 type-2A fractures, 10 type-2B fractures, and 11 type-3 fractures. The mean Olerud-Molander Ankle Score was 75.9 points (95% confidence interval [CI], 66.4 to 85.3 points) for patients with type-1 fractures, 75.0 points (95% CI, 61.5 to 88.5 points) for patients with type-2A fractures, 74.0 points (95% CI, 64.2 to 83.8 points) for patients with type-2B fractures, and 70.5 points (95% CI, 59.0 to 81.9 points) for patients with type-3 fractures.
Conclusions: We have been able to demonstrate an improvement in the Olerud-Molander Ankle Score for all posterior malleolar fractures with the treatment algorithm applied using the Mason and Molloy classification. Mason classification type-3 fractures have marginally poorer outcomes, which correlates with a more severe injury; however, this did not reach significance.
Level of evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Nelson MC, Jensen NK. The treatment of trimalleolar fractures of the ankle. Surg Gynecol Obstet. 1940;71:509-14.
-
- Odak S, Ahluwalia R, Unnikrishnan P, Hennessy M, Platt S. Management of posterior malleolar fractures: a systematic review. J Foot Ankle Surg. 2016. Jan-Feb;55(1):140-5. Epub 2015 Jun 19. - PubMed
-
- Veltman ES, Halma JJ, de Gast A. Longterm outcome of 886 posterior malleolar fractures: a systematic review of the literature. Foot Ankle Surg. 2016. June;22(2):73-7. Epub 2015 May 28. - PubMed
-
- Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006. May;88(5):1085-92. - PubMed
-
- Mangnus L, Meijer DT, Stufkens SA, Mellema JJ, Steller EP, Kerkhoffs GM, Doornberg JN. Posterior malleolar fracture patterns. J Orthop Trauma. 2015. September;29(9):428-35. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials