

The impact of infection and inflammation in oncologic 18F-FDG PET/CT imaging
- PMID: 31334700
- PMCID: PMC7104808
- DOI: 10.1016/j.biopha.2019.109168
The impact of infection and inflammation in oncologic 18F-FDG PET/CT imaging
Abstract
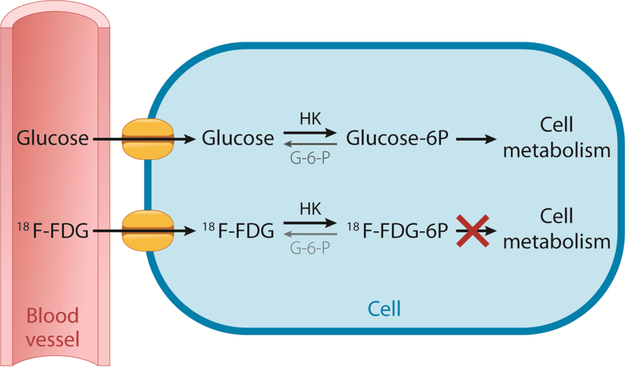
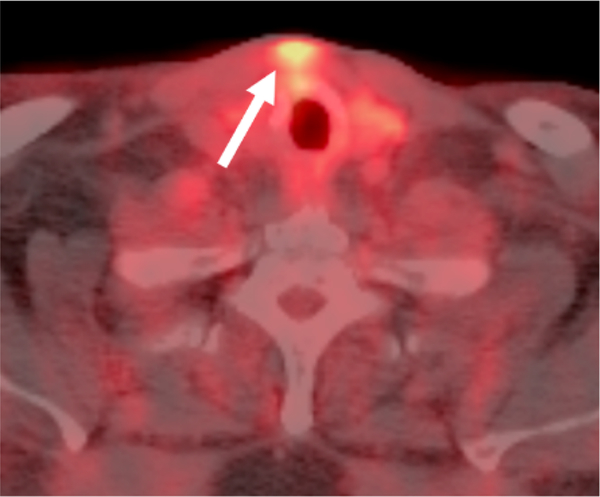
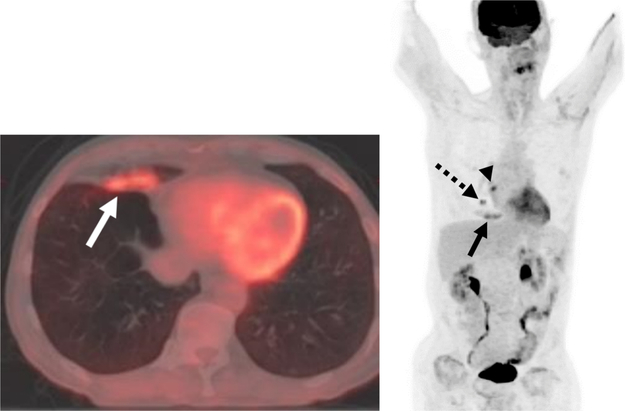
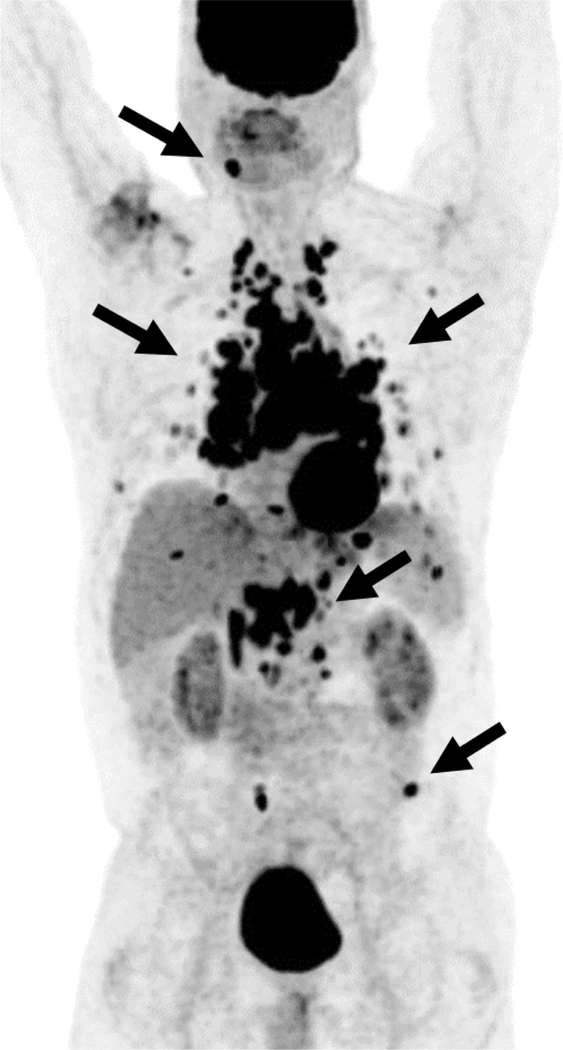
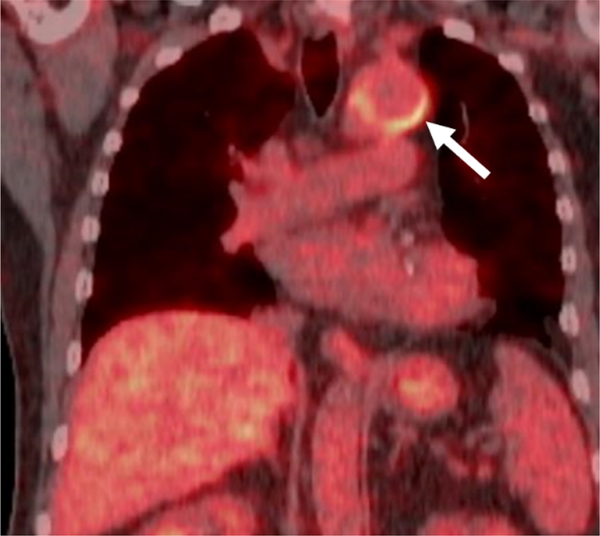
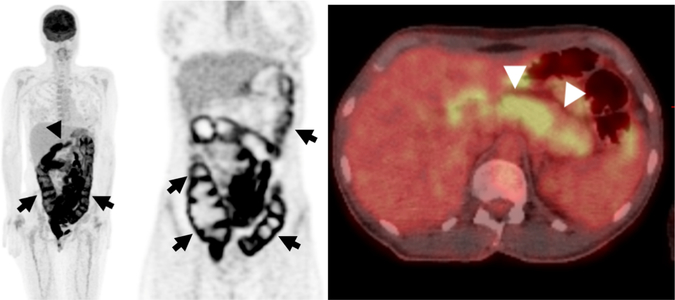
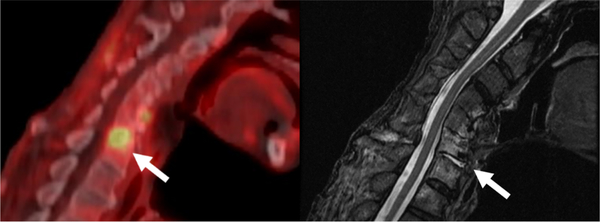
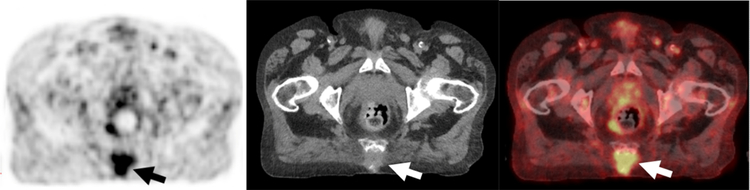
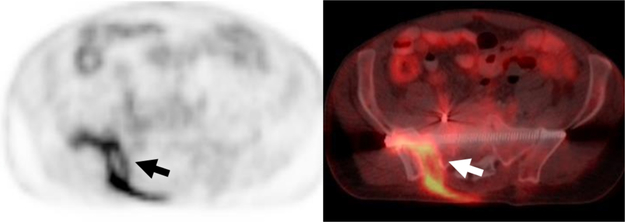
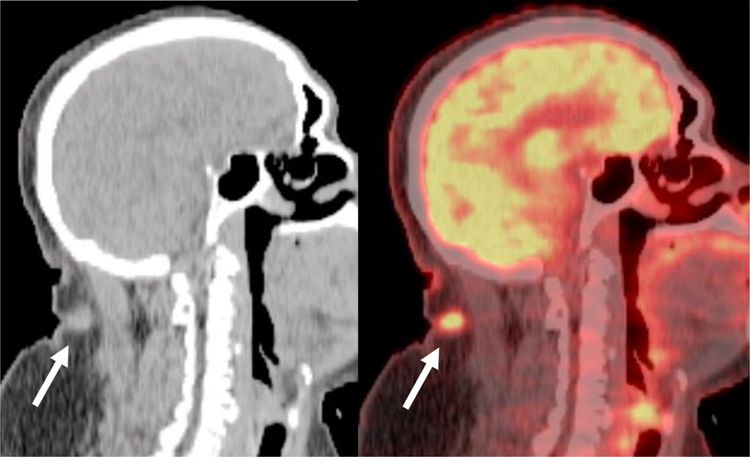
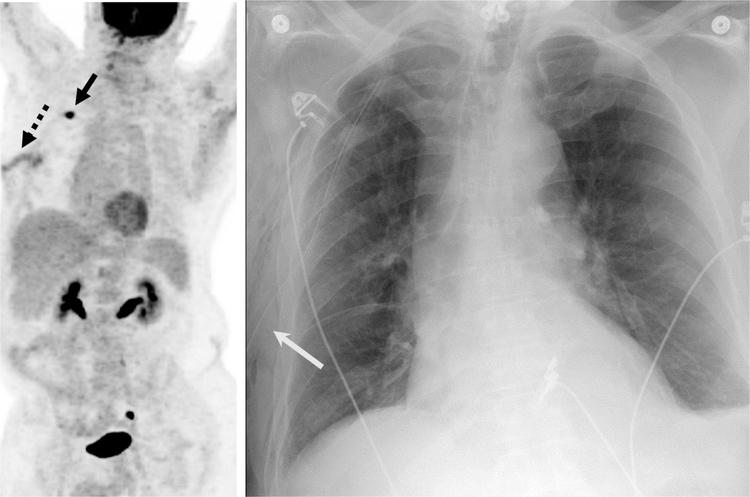
Sites of infection and inflammation can be misleading in oncology PET/CT imaging because these areas commonly show 18F-FDG activity. Caution in the interpretation must be taken to avoid the misdiagnosis of malignancy. Utilization of both CT findings as well as patient history can help differentiate benign infectious and inflammatory processes from malignancy, although occasionally additional work-up may be required. This article discusses the mechanism of 18F-FDG uptake in infection and inflammation with illustrative examples.
Keywords: (18)F-FDG PET/CT; Imaging pitfalls; Infection; Inflammation.
Copyright © 2019 The Authors. Published by Elsevier Masson SAS.. All rights reserved.
Figures

References
-
- Safaie E, Matthews R, Bergamaschi R, PET scan findings can be false positive, Tech. Coloproctol 19 (6) (2015) 329–330. - PubMed
-
- Annibaldi A, Widmann C, Glucose metabolism in cancer cells, Curr. Opin. Clin. Nutr. Metab. Care 13 (4) (2010) 466–470. - PubMed
-
- Gallagher BM, Fowler JS, Gutterson NI, MacGregor RR, Wan CN, Wolf AP, Metabolic trapping as a principle of oradiopharmaceutical design: some factors resposible for the biodistribution of [18F] 2-deoxy-2-fluoro-D-glucose, J. Nucl. Med 19 (10) (1978) 1154–1161. - PubMed
-
- Smith TA, FDG uptake, tumour characteristics and response to therapy: a review, Nucl. Med. Commun 19 (2) (1998) 97–105. - PubMed
-
- Vaidyanathan S, Patel CN, Scarsbrook AF, Chowdhury FU, FDG PET/CT in infection and inflammation–current and emerging clinical applications, Clin. Radiol 70 (7) (2015) 787–800. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
