

doi: 10.14309/ctg.0000000000000067.
Primer on Precision Medicine for Complex Chronic Disorders
Affiliations
- PMID: 31335357
- PMCID: PMC6708660
- DOI: 10.14309/ctg.0000000000000067
Item in Clipboard
Primer on Precision Medicine for Complex Chronic Disorders
Clin Transl Gastroenterol.
2019 Jul.
Abstract
Precision medicine promises patients with complex disorders the right treatment for the right patient at the right dose at the right time with expectation of better health at a lower cost. The demand for precision medicine highlights the limitations of modern Western medicine. Modern Western medicine is a population-based, top-down approach that uses pathology to define disease. Precision medicine is a bottom-up approach that identifies predisease disorders using genetics, biomarkers, and modeling to prevent disease. This primer demonstrates the contrasting strengths and limitations of each paradigm and why precision medicine will eventually deliver on the promises.
Figures
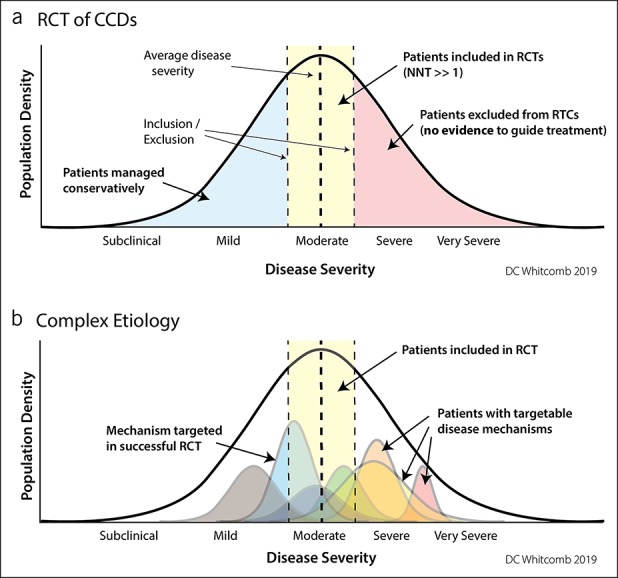
Therapeutic trials using clinicopathologic disease criteria. (a) Randomized clinical trials attempt to reduce heterogeneity by selecting the maximum number of patients with the least variability in disease features using inclusion–exclusion criteria. In CCDs, the treatment response is mixed with the NNT >>1. The patients with the highest burden of disease and in need of effective treatment are excluded from traditional clinical drug trials. (b) The same disease population seen as a function of multiple underlying disorders (colored curves) that may be a function of a single or multiple factors. A RCT targeting a low-severity mechanism (blue curve) will have “strong evidence” of effectiveness in the RCT, but will be of no value in more severe disease mechanisms (yellow, orange, and red curves). New approaches are needed to apply drug trials to mechanisms rather than common symptoms. CCD, complex chronic diseases; NNT, number needed to treat; RCT, randomized controlled trial.
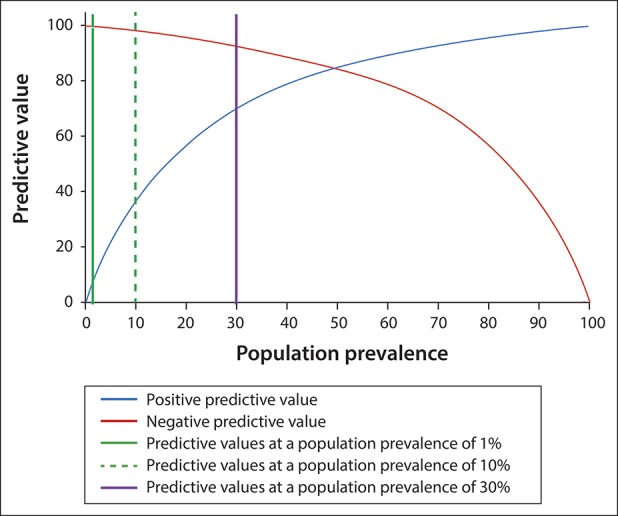
Effect of defining genetic risk factors in defined subpopulations to improve biomarker performance. In this example (a biomarker with a sensitivity of 85% and specificity of 85%), the identification of high-risk genetic risk factors moves a patient from a low-risk population (e.g., 1% prevalence) or patients with some disease symptoms (10% prevalence) to a subpopulation of patients with a high disease prevalence (e.g., 30%). Knowing the underlying mechanistic disorder through genetic analysis also adds specificity and also provides possible treatment targets.
References
-
- National Center for Chronic Disease Prevention and Health Promotion. Health and Economic Costs of Chronic Diseases (https://www.cdc.gov/chronicdisease/about/costs/index.htm) (2019). Accessed March 4, 2019.
-
- Atkinson AJJ, Colburn WA, DeGruttola VG, et al. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin Pharmacol Ther 2001;69(3):89–95. - PubMed
-
- Beck AH. STUDENT JAMA. The Flexner report and the standardization of American medical education. JAMA 2004;291(17):2139–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
