

Major Neurologic Complications Associated With Postdural Puncture Headache in Obstetrics: A Retrospective Cohort Study
- PMID: 31335402
- PMCID: PMC9924132
- DOI: 10.1213/ANE.0000000000004336
Major Neurologic Complications Associated With Postdural Puncture Headache in Obstetrics: A Retrospective Cohort Study
Abstract
Background: Increased risks of cerebral venous thrombosis or subdural hematoma, bacterial meningitis, persistent headache, and persistent low back pain are suggested in obstetric patients with postdural puncture headache (PDPH). Acute postpartum pain such as PDPH may also lead to postpartum depression. This study tested the hypothesis that PDPH in obstetric patients is associated with significantly increased postpartum risks of major neurologic and other maternal complications.
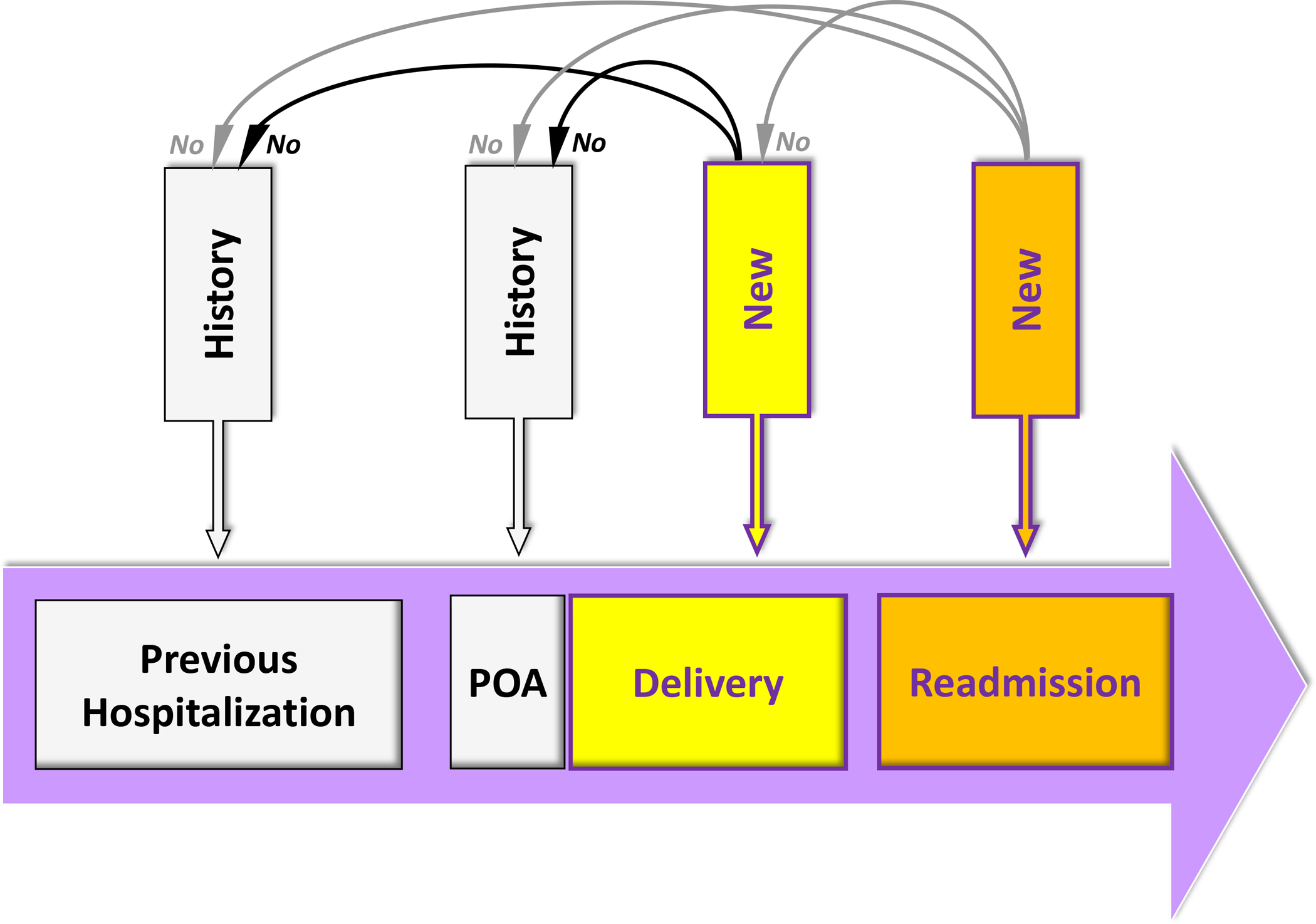
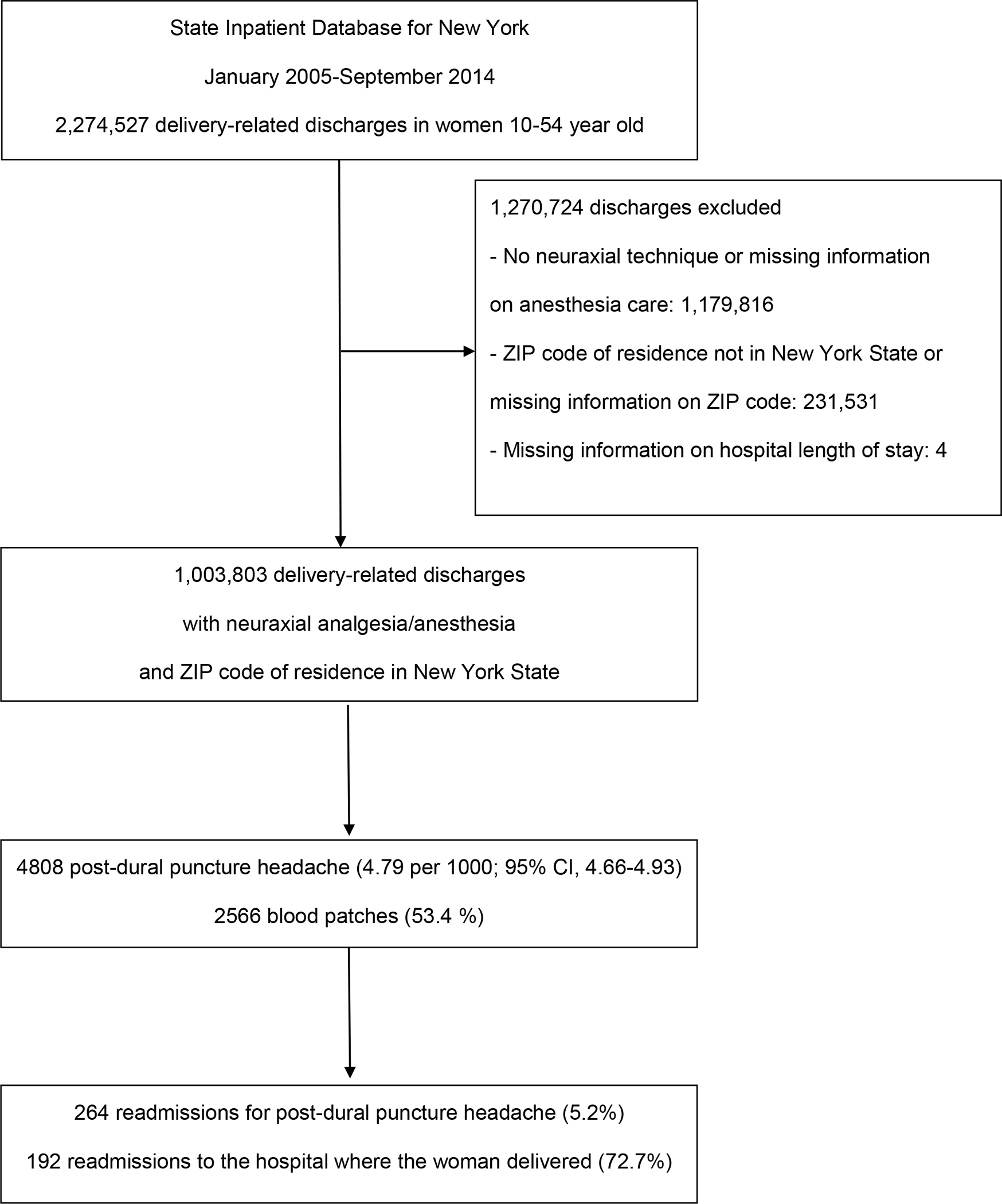
Methods: This retrospective cohort study consisted of 1,003,803 women who received neuraxial anesthesia for childbirth in New York State hospitals between January 2005 and September 2014. The primary outcome was the composite of cerebral venous thrombosis and subdural hematoma. The 4 secondary outcomes were bacterial meningitis, depression, headache, and low back pain. PDPH and complications were identified during the delivery hospitalization and up to 1 year postdelivery. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were estimated using the inverse probability of treatment weighting approach.
Results: Of the women studied, 4808 (0.48%; 95% CI, 0.47-0.49) developed PDPH, including 264 cases (5.2%) identified during a readmission with a median time to readmission of 4 days. The incidence of cerebral venous thrombosis and subdural hematoma was significantly higher in women with PDPH than in women without PDPH (3.12 per 1000 neuraxial or 1:320 vs 0.16 per 1000 or 1:6250, respectively; P < .001). The incidence of the 4 secondary outcomes was also significantly higher in women with PDPH than in women without PDPH. The aORs associated with PDPH were 19.0 (95% CI, 11.2-32.1) for the composite of cerebral venous thrombosis and subdural hematoma, 39.7 (95% CI, 13.6-115.5) for bacterial meningitis, 1.9 (95% CI, 1.4-2.6) for depression, 7.7 (95% CI, 6.5-9.0) for headache, and 4.6 (95% CI, 3.3-6.3) for low back pain. Seventy percent of cerebral venous thrombosis and subdural hematoma were identified during a readmission with a median time to readmission of 5 days.
Conclusions: PDPH is associated with substantially increased postpartum risks of major neurologic and other maternal complications, underscoring the importance of early recognition and treatment of anesthesia-related complications in obstetrics.
Conflict of interest statement
Figures
Comment in
-
Is Insufficient Evidence Sufficient?Anesth Analg. 2019 Nov;129(5):1202-1204. doi: 10.1213/ANE.0000000000004437. Anesth Analg. 2019. PMID: 31613810 No abstract available.
-
In Response.Anesth Analg. 2020 Feb;130(2):e41-e42. doi: 10.1213/ANE.0000000000004527. Anesth Analg. 2020. PMID: 31764155 No abstract available.
-
The Dilemma of Treating Postdural Puncture Headache.Anesth Analg. 2020 Feb;130(2):e41. doi: 10.1213/ANE.0000000000004526. Anesth Analg. 2020. PMID: 31764162 No abstract available.
References
-
- D’Angelo R, Smiley RM, Riley ET, Segal S. Serious complications related to obstetric anesthesia. Anesthesiology 2014;120:1005–12. - PubMed
-
- Macarthur A. Postpartum headache. In: Chestnut DH, ed. Chestnut’s obstetric anesthesia: Principles and practice. Fifth edition ed. Philadelphia, PA: Elsevier Saunders, 2014:713–38.
-
- McQuaid-Hanson E, Hopp S, Radoslovich S, Leffert L, Bateman B. Risk factors and indications for postpartum readmission: A retrospective cohort study (Abstract #O2–03). Society for Obstetric Anesthesia and Perinatalogy 48th Annual Meeting. Boston, 2016.
-
- Davies JM, Posner KL, Lee LA, Cheney FW, Domino KB. Liability associated with obstetric anesthesia: A closed claims analysis. Anesthesiology 2009;110:131–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
