

Compensatory Neural Recruitment for Error-Related Cerebral Activity in Patients with Moderate-To-Severe Obstructive Sleep Apnea
- PMID: 31336598
- PMCID: PMC6678110
- DOI: 10.3390/jcm8071077
Compensatory Neural Recruitment for Error-Related Cerebral Activity in Patients with Moderate-To-Severe Obstructive Sleep Apnea
Abstract
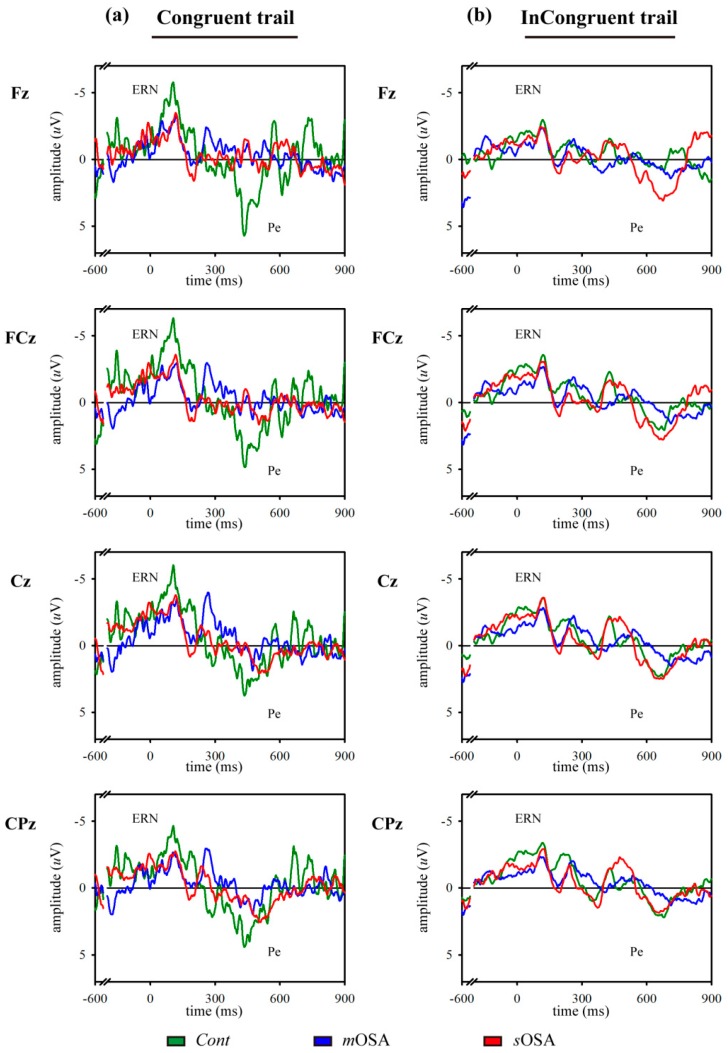
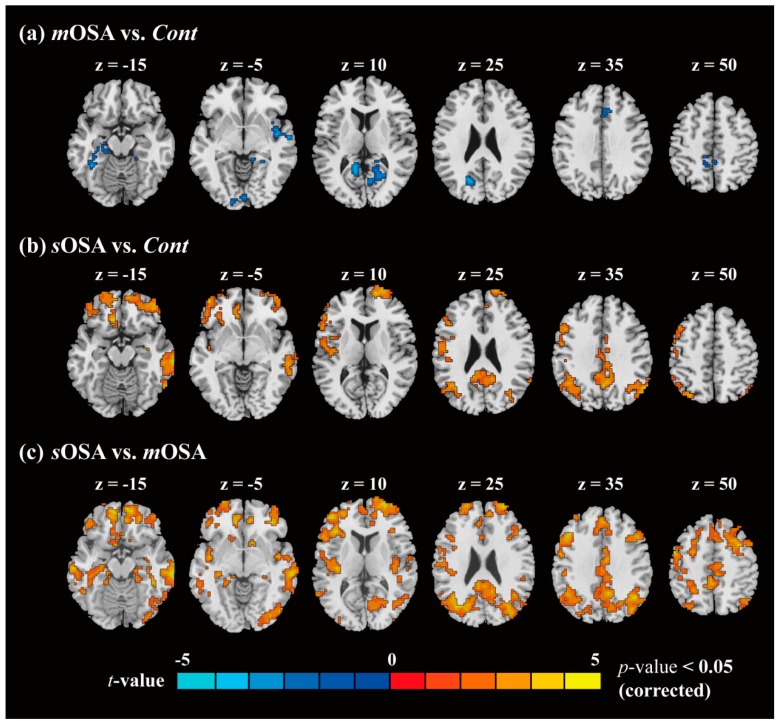
(1) Background: Although it is known that obstructive sleep apnea (OSA) impairs action-monitoring function, there is only limited information regarding the associated cerebral substrate underlying this phenomenon. (2) Methods: The modified Flanker task, error-related event-related potentials (ERPs), namely, error-related negativity (ERN) and error positivity (Pe), and functional magnetic resonance imaging (fMRI) were used to evaluate neural activities and the functional connectivity underlying action-monitoring dysfunction in patients with different severities of OSA. (3) Results: A total of 14 control (Cont) subjects, 17 patients with moderate OSA (mOSA), and 10 patients with severe OSA (sOSA) were enrolled. A significant decline in posterror correction rate was observed in the modified Flanker task when patients with mOSA were compared with Cont subjects. Comparison between patients with mOSA and sOSA did not reveal any significant difference. In the analysis of ERPs, ERN and Pe exhibited declined amplitudes in patients with mOSA compared with Cont subjects, which were found to increase in patients with sOSA. Results of fMRI revealed a decreased correlation in multiple anterior cingulate cortex functional-connected areas in patients with mOSA compared with Cont subjects. However, these areas appeared to be reconnected in patients with sOSA. (4) Conclusions: The behavioral, neurophysiological, and functional image findings obtained in this study suggest that mOSA leads to action-monitoring dysfunction; however, compensatory neural recruitment might have contributed to the maintenance of the action-monitoring function in patients with sOSA.
Keywords: action monitoring; error positivity; error-related negativity; functional magnetic resonance imaging; modified Flanker task; obstructive sleep apnea.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
