

Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies
- PMID: 31336859
- PMCID: PMC6679311
- DOI: 10.3390/cancers11070976
Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies
Abstract
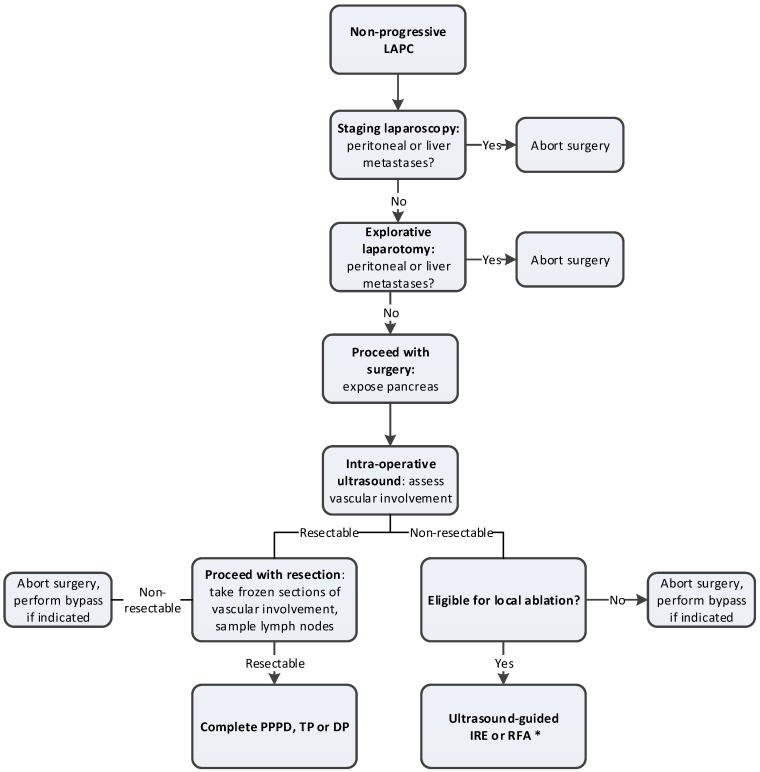
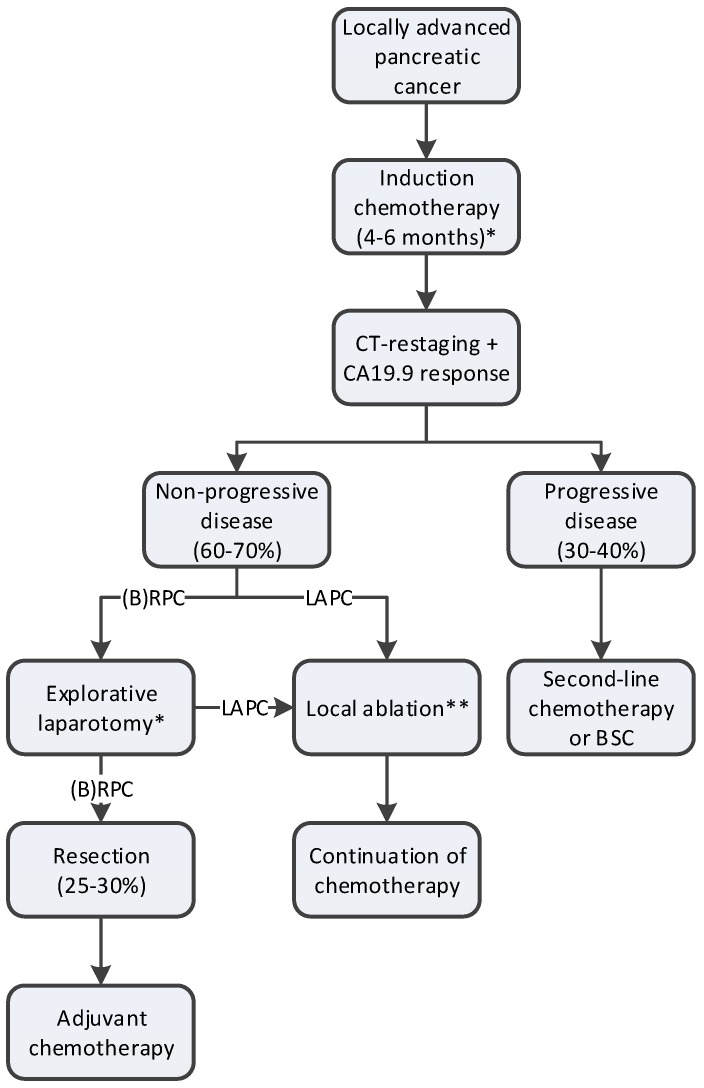
Locally advanced pancreatic cancer (LAPC) has several definitions but essentially is a nonmetastasized pancreatic cancer, in which upfront resection is considered not beneficial due to extensive vascular involvement and consequent high chance of a nonradical resection. The introduction of FOLFIRINOX chemotherapy and gemcitabine-nab-paclitaxel (gem-nab) has had major implications for the management and outcome of patients with LAPC. After 4-6 months induction chemotherapy, the majority of patients have stable disease or even tumor-regression. Of these, 12 to 35% are successfully downstaged to resectable disease. Several studies have reported a 30-35 months overall survival after resection; although it currently remains unclear if this is a result of the resection or the good response to chemotherapy. Following chemotherapy, selection of patients for resection is difficult, as contrast-enhanced computed-tomography (CT) scan is unreliable in differentiating between viable tumor and fibrosis. In case a resection is not considered possible but stable disease is observed, local ablative techniques are being studied, such as irreversible electroporation, radiofrequency ablation, and stereotactic body radiation therapy. Pragmatic, multicenter, randomized studies will ultimately have to confirm the exact role of both surgical exploration and ablation in these patients. Since evidence-based guidelines for the management of LAPC are lacking, this review proposes a standardized approach for the treatment of LAPC based on the best available evidence.
Keywords: FOLFIRINOX; ablation; explorative laparotomy; locally advanced pancreatic cancer; resection.
Conflict of interest statement
M.R.M. and K.P.v.L. are paid consultants for AngioDynamics®. The other authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Ferlay J., Soerjomataram I., Ervik M., Dikshit R., Eser S., Mathers C., Rebelo M., Parkin D.M., Forman D., Bray F. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. International Agency for Research on Cancer; Lyon, France: 2014.
-
- Ducreux M., Cuhna A.S., Caramella C., Hollebecque A., Burtin P., Goere D., Seufferlein T., Haustermans K., Van Laethem J.L., Conroy T., et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015;26(Suppl. 5):v56–v68. doi: 10.1093/annonc/mdv295. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
