Influences of the biofeedback content on robotic post-stroke gait rehabilitation: electromyographic vs joint torque biofeedback
- PMID: 31337400
- PMCID: PMC6652021
- DOI: 10.1186/s12984-019-0558-0
Influences of the biofeedback content on robotic post-stroke gait rehabilitation: electromyographic vs joint torque biofeedback
Abstract
Background: Add-on robot-mediated therapy has proven to be more effective than conventional therapy alone in post-stroke gait rehabilitation. Such robot-mediated interventions routinely use also visual biofeedback tools. A better understanding of biofeedback content effects when used for robotic locomotor training may improve the rehabilitation process and outcomes.
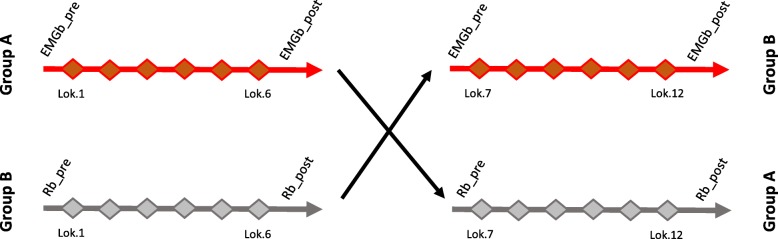
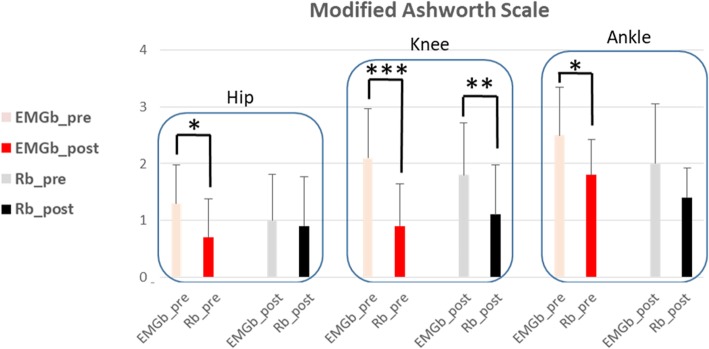
Methods: This randomized cross-over pilot trial aimed to address the possible impact of different biofeedback contents on patients' performance and experience during Lokomat training, by comparing a novel biofeedback based on online biological electromyographic information (EMGb) versus the commercial joint torque biofeedback (Rb) in sub-acute non ambulatory patients. 12 patients were randomized into two treatment groups, A and B, based on two different biofeedback training. For both groups, study protocol consisted of 12 Lokomat sessions, 6 for each biofeedback condition, 40 min each, 3 sessions per week of frequency. All patients performed Lokomat trainings as an add-on therapy to the conventional one that was the same for both groups and consisted of 40 min per day, 5 days per week. The primary outcome was the Modified Ashworth Spasticity Scale, and secondary outcomes included clinical, neurological, mechanical, and personal experience variables collected before and after each biofeedback training.
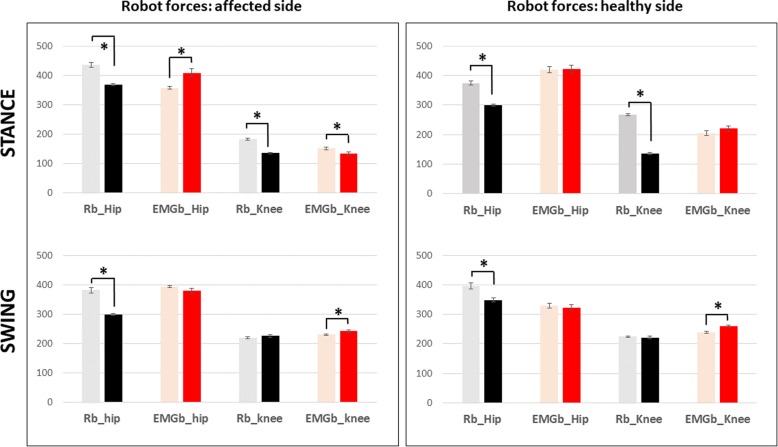
Results: Lokomat training significantly improved gait/daily living activity independence and trunk control, nevertheless, different effects due to biofeedback content were remarked. EMGb was more effective to reduce spasticity and improve muscle force at the ankle, knee and hip joints. Robot data suggest that Rb induces more adaptation to robotic movements than EMGb. Furthermore, Rb was perceived less demanding than EMGb, even though patient motivation was higher for EMGb. Robot was perceived to be effective, easy to use, reliable and safe: acceptability was rated as very high by all patients.
Conclusions: Specific effects can be related to biofeedback content: when muscular-based information is used, a more direct effect on lower limb spasticity and muscle activity is evidenced. In a similar manner, when biofeedback treatment is based on joint torque data, a higher patient compliance effect in terms of force exerted is achieved. Subjects who underwent EMGb seemed to be more motivated than those treated with Rb.
Keywords: Biofeedback; Biomechanics; Electromyography; Rehabilitation; Robot; Stroke; Top-down approach.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures