

Delirium detection in older acute medical inpatients: a multicentre prospective comparative diagnostic test accuracy study of the 4AT and the confusion assessment method
- PMID: 31337404
- PMCID: PMC6651960
- DOI: 10.1186/s12916-019-1367-9
Delirium detection in older acute medical inpatients: a multicentre prospective comparative diagnostic test accuracy study of the 4AT and the confusion assessment method
Abstract
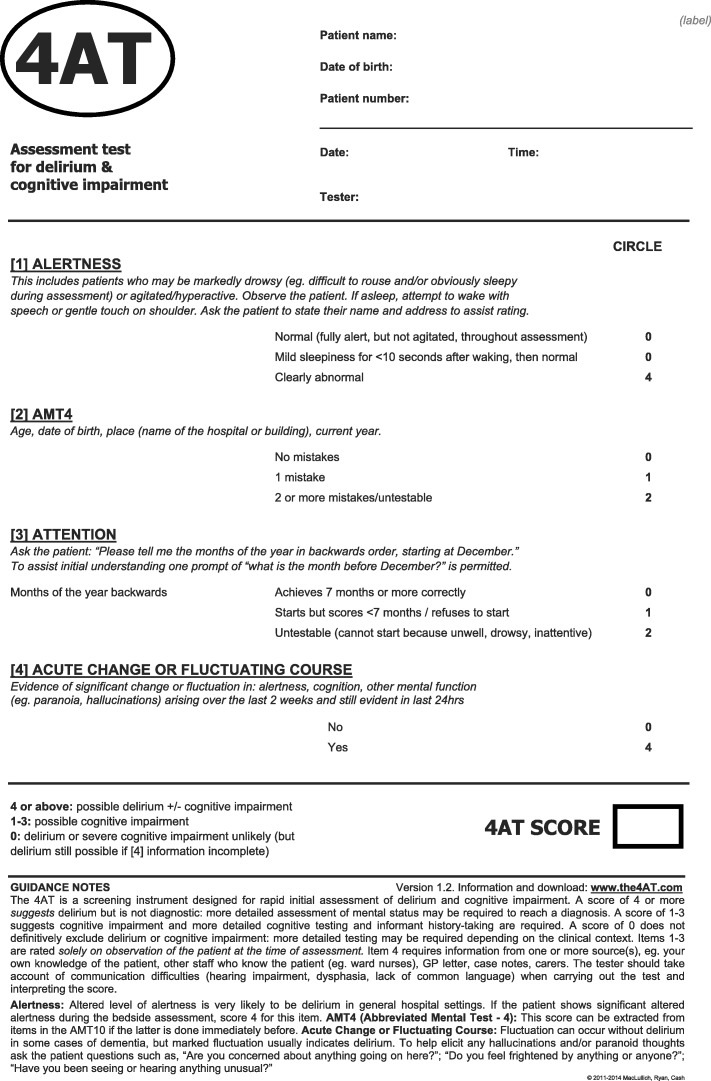
Background: Delirium affects > 15% of hospitalised patients but is grossly underdetected, contributing to poor care. The 4 'A's Test (4AT, www.the4AT.com ) is a short delirium assessment tool designed for routine use without special training. The primary objective was to assess the accuracy of the 4AT for delirium detection. The secondary objective was to compare the 4AT with another commonly used delirium assessment tool, the Confusion Assessment Method (CAM).
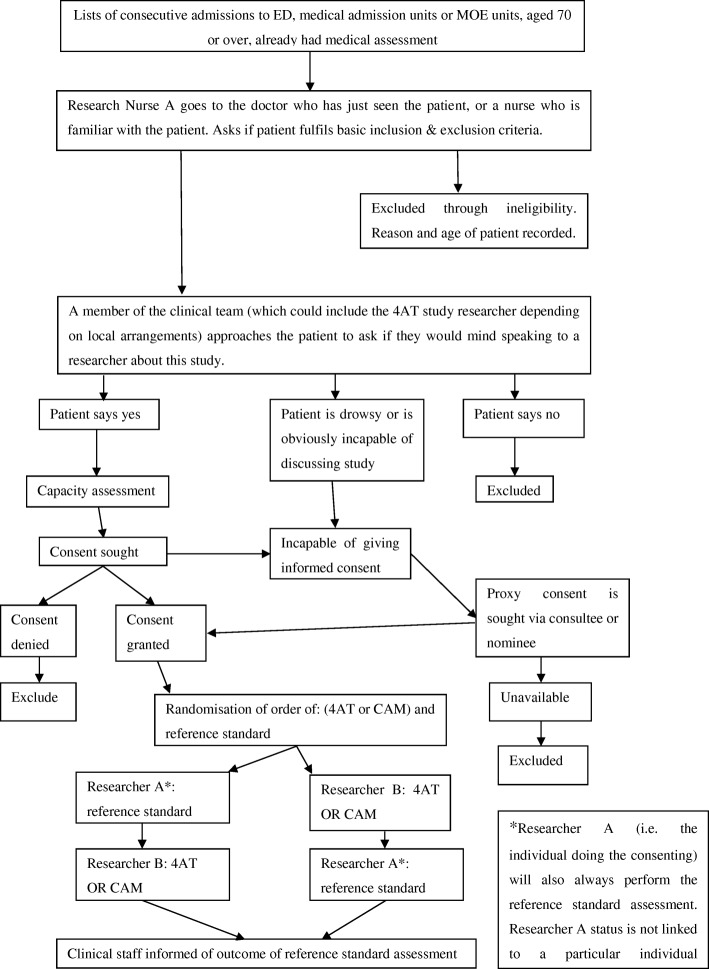
Methods: This was a prospective diagnostic test accuracy study set in emergency departments or acute medical wards involving acute medical patients aged ≥ 70. All those without acutely life-threatening illness or coma were eligible. Patients underwent (1) reference standard delirium assessment based on DSM-IV criteria and (2) were randomised to either the index test (4AT, scores 0-12; prespecified score of > 3 considered positive) or the comparator (CAM; scored positive or negative), in a random order, using computer-generated pseudo-random numbers, stratified by study site, with block allocation. Reference standard and 4AT or CAM assessments were performed by pairs of independent raters blinded to the results of the other assessment.
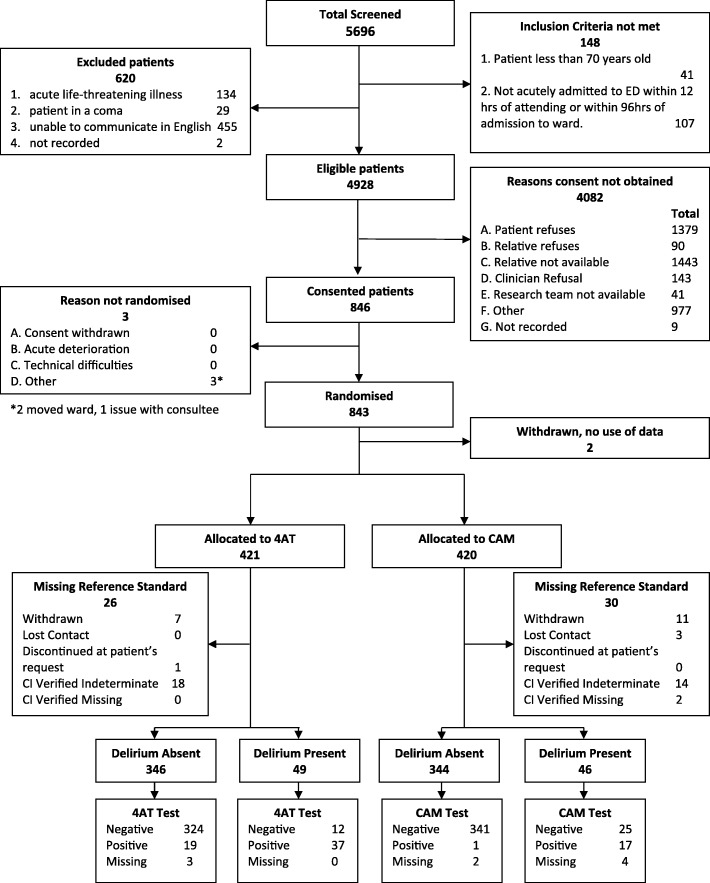
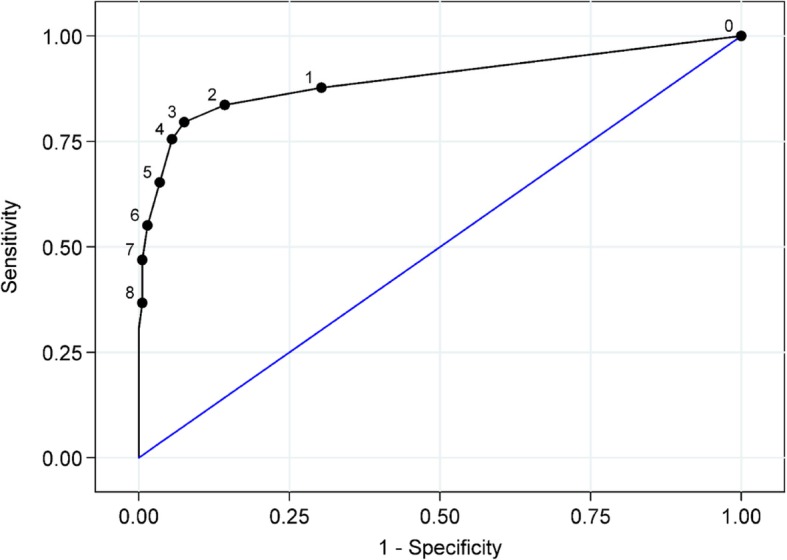
Results: Eight hundred forty-three individuals were randomised: 21 withdrew, 3 lost contact, 32 indeterminate diagnosis, 2 missing outcome, and 785 were included in the analysis. Mean age was 81.4 (SD 6.4) years. 12.1% (95/785) had delirium by reference standard assessment, 14.3% (56/392) by 4AT, and 4.7% (18/384) by CAM. The 4AT had an area under the receiver operating characteristic curve of 0.90 (95% CI 0.84-0.96). The 4AT had a sensitivity of 76% (95% CI 61-87%) and a specificity of 94% (95% CI 92-97%). The CAM had a sensitivity of 40% (95% CI 26-57%) and a specificity of 100% (95% CI 98-100%).
Conclusions: The 4AT is a short, pragmatic tool which can help improving detection rates of delirium in routine clinical care.
Trial registration: International standard randomised controlled trial number (ISRCTN) 53388093 . Date applied 30/05/2014; date assigned 02/06/2014.
Keywords: 4AT; Confusion assessment method (CAM); Delirium; Diagnostic test accuracy; Hospital; Sensitivity; Specificity.
Conflict of interest statement
AMJM led the design of the 4AT in 2011 (with others, see
Figures
References
-
- Reynish EL, Hapca SM, De Souza N, Cvoro V, Donnan PT, Guthrie B. Epidemiology and outcomes of people with dementia, delirium, and unspecified cognitive impairment in the general hospital: prospective cohort study of 10,014 admissions. BMC Med. 2017;15(1):140. doi: 10.1186/s12916-017-0899-0. - DOI - PMC - PubMed
-
- Pendlebury ST, Lovett NG, Smith SC, Dutta N, Bendon C, Lloyd-Lavery A, Mehta Z, Rothwell PM. Observational, longitudinal study of delirium in consecutive unselected acute medical admissions: age-specific rates and associated factors, mortality and re-admission. BMJ open. 2015;5(11):e007808. doi: 10.1136/bmjopen-2015-007808. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
