

Durable Long-Term Bacterial Engraftment following Encapsulated Fecal Microbiota Transplantation To Treat Clostridium difficile Infection
- PMID: 31337728
- PMCID: PMC6650559
- DOI: 10.1128/mBio.01586-19
Durable Long-Term Bacterial Engraftment following Encapsulated Fecal Microbiota Transplantation To Treat Clostridium difficile Infection
Abstract
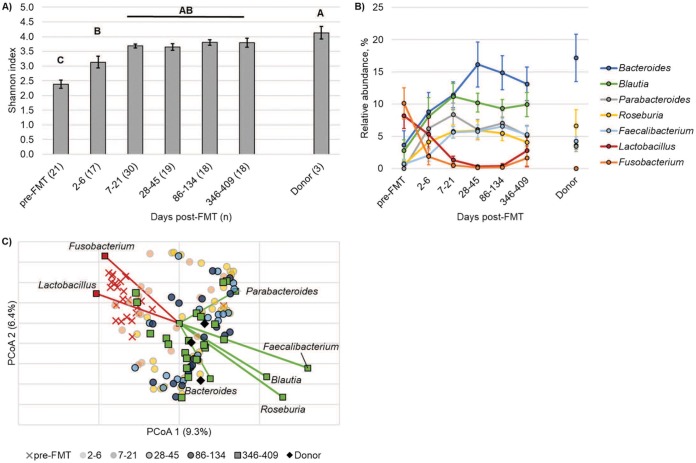
Fecal microbiota transplantation (FMT) has become a common rescue therapy for recurrent Clostridium difficile infection, and encapsulated delivery (cFMT) of healthy donor microbiota shows similar clinical efficacy as more traditional routes of administration. In this study, we characterized long-term patterns of bacterial engraftment in a cohort of 18 patients, who received capsules from one of three donors, up to 409 days post-FMT. Bacterial communities were characterized using Illumina sequencing of the V5-V6 hypervariable regions of the 16S rRNA gene, and engraftment was determined by using the Bayesian algorithm SourceTracker. All patients recovered clinically and were free of C. difficile infection following cFMT. The majority of patients (61%) showed high levels of engraftment after the first week following FMT, which were sustained throughout the year. A small subset, 22%, experienced a decline in donor engraftment after approximately 1 month, and a few patients (17%), two of whom were taking metformin, showed delayed and low levels of donor engraftment. Members of the genera Bacteroides, Parabacteroides, and Faecalibacterium were significantly and positively correlated with donor similarity (ρ = 0.237 to 0.373, P ≤ 0.017). Furthermore, throughout the year, patient fecal communities showed significant separation based on the donor fecal microbiota that they received (P < 0.001). Results of this study, which characterize long-term engraftment following cFMT, suggest that numerical donor similarity is not strictly related to clinical outcome and identify a persistent donor-specific effect on patient fecal microbial communities. Furthermore, results suggest that members of the Bacteroidetes may be important targets to improve engraftment via cFMT.IMPORTANCE Recurrent Clostridium difficile infection (rCDI) is the most common cause of hospital- and community-acquired diarrheal infection associated with antibiotic use. Fecal microbiota transplantation (FMT), a treatment that involves administration of fecal bacteria from a healthy donor to a recipient patient, is a highly effective rescue therapy for rCDI that is increasingly being incorporated into standard clinical practice. Encapsulated, freeze-dried preparations of fecal microbiota, administered orally, offer the simplest and most convenient route of FMT delivery for patients (cFMT). In this study, we evaluated the extent of bacterial engraftment following cFMT and the duration of donor bacterial persistence. All patients studied recovered clinically but showed differing patterns in long-term microbial community similarity to the donor that were associated with members of the bacterial group Bacteroidetes, previously shown to be prominent contributors to rCDI resistance. Results highlight long-lasting, donor-specific effects on recipient patient microbiota and reveal potential bacterial targets to improve cFMT engraftment.
Keywords: Bacteroides; capsule FMT; donor; engraftment; fecal transplant; stable.
Copyright © 2019 Staley et al.
Figures




References
-
- Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. 2015. Burden of Clostridium difficile infection in the United States. N Engl J Med 372:825–834. doi: 10.1056/NEJMoa1408913. - DOI - PMC - PubMed
-
- McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, Dubberke ER, Garey KW, Gould CV, Kelly C, Loo V, Shaklee Sammons J, Sandora TJ, Wilcox MH. 2018. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 66:987–994. doi: 10.1093/cid/ciy149. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
