

Diversity in the emergency care for febrile children in Europe: a questionnaire study
- PMID: 31338429
- PMCID: PMC6613846
- DOI: 10.1136/bmjpo-2019-000456
Diversity in the emergency care for febrile children in Europe: a questionnaire study
Abstract
Objective: To provide an overview of care in emergency departments (EDs) across Europe in order to interpret observational data and implement interventions regarding the management of febrile children.
Design and setting: An electronic questionnaire was sent to the principal investigators of an ongoing study (PERFORM (Personalised Risk assessment in Febrile illness to Optimise Real-life Management), www.perform2020.eu) in 11 European hospitals in eight countries: Austria, Germany, Greece, Latvia, the Netherlands, Slovenia, Spain and the UK.
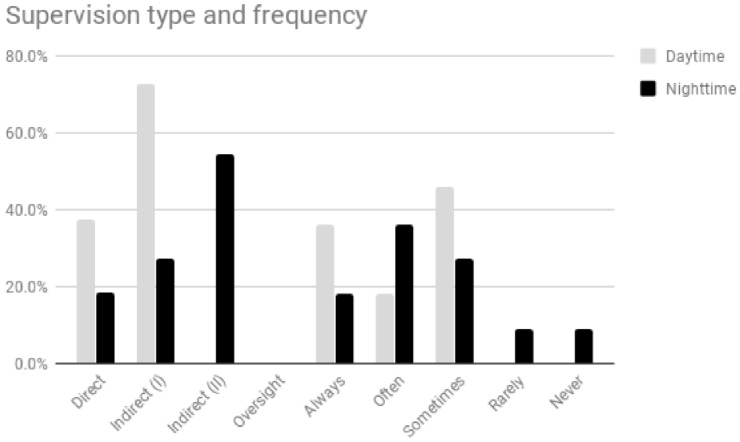
Outcome measures: The questionnaire covered indicators in three domains: local ED quality (supervision, guideline availability, paper vs electronic health records), organisation of healthcare (primary care, immunisation), and local factors influencing or reflecting resource use (availability of point-of-care tests, admission rates).
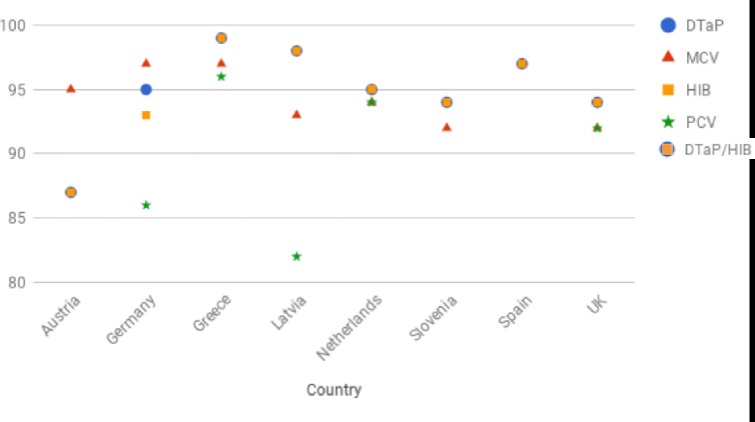
Results: Reported admission rates ranged from 4% to 51%. In six settings (Athens, Graz, Ljubljana, Riga, Rotterdam, Santiago de Compostela), the supervising ED physicians were general paediatricians, in two (Liverpool, London) these were paediatric emergency physicians, in two (Nijmegen, Newcastle) supervision could take place by either a general paediatrician or a general emergency physician, and in one (München) this could be either a general paediatrician or a paediatric emergency physician. The supervising physician was present on site in all settings during office hours and in five out of eleven settings during out-of-office hours. Guidelines for fever and sepsis were available in all settings; however, the type of guideline that was used differed. Primary care was available in all settings during office hours and in eight during out-of-office hours. There were differences in routine immunisations as well as in additional immunisations that were offered; immunisation rates varied between and within countries.
Conclusion: Differences in local, regional and national aspects of care exist in the management of febrile children across Europe. This variability has to be considered when trying to interpret differences in the use of diagnostic tools, antibiotics and admission rates. Any future implementation of interventions or diagnostic tests will need to be aware of this European diversity.
Keywords: accident & emergency; infectious diseases.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- parliament.uk Available: http://researchbriefings.parliament.uk/ResearchBriefing/Summary/CBP-7281 [Accessed 10 Nov 2017].