

Ileostomy for steroid-resistant acute graft-versus-host disease of the gastrointestinal tract
- PMID: 31338570
- PMCID: PMC7101733
- DOI: 10.1007/s00277-019-03754-3
Ileostomy for steroid-resistant acute graft-versus-host disease of the gastrointestinal tract
Abstract
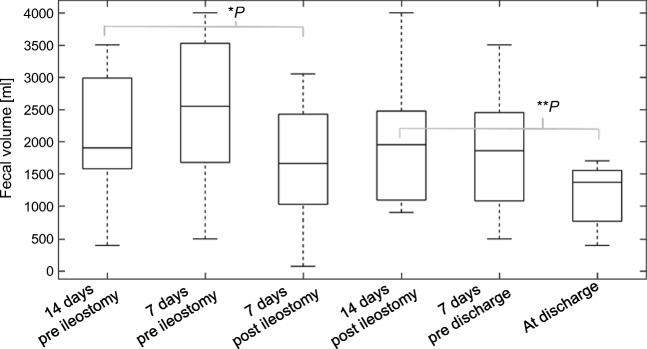
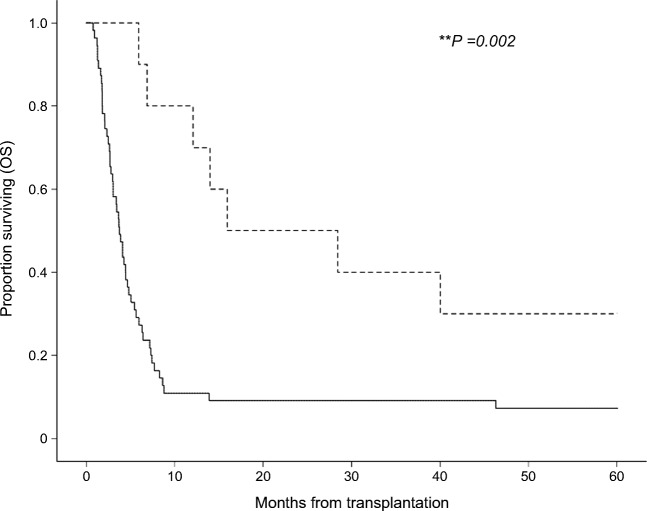
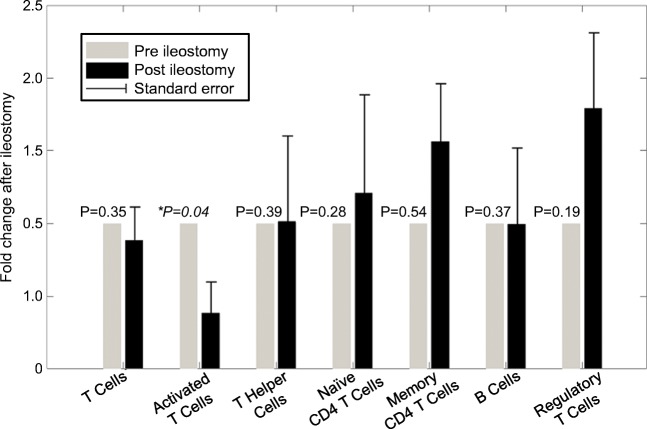
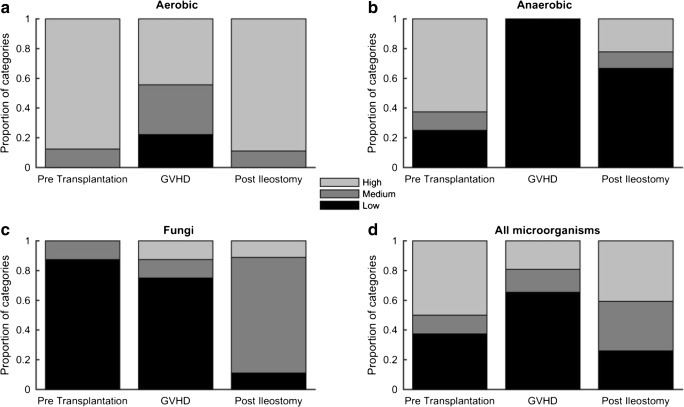
Steroid-resistant acute graft-versus-host disease (GVHD) of the gastrointestinal tract associates with important morbidity and mortality. While high-dose steroids are the established first-line therapy in GVHD, no second-line therapy is generally accepted. In this analysis of 65 consecutive patients with severe, steroid-resistant, intestinal GVHD (92% stage 4), additional ileostomy surgery significantly reduced overall mortality (hazard ratio 0.54; 95% confidence interval, 0.36-0.81; p = 0.003) compared to conventional GVHD therapy. Median overall survival was 16 months in the ileostomy cohort compared to 4 months in the conventional therapy cohort. In the ileostomy cohort, both infectious- and GVHD-associated mortality were reduced (40% versus 77%). Significantly declined fecal volumes (p = 0.001) after surgery provide evidence of intestinal adaptation following ileostomy. Correlative studies indicated ileostomy-induced immune-modulation with a > 50% decrease of activated T cells (p = 0.04) and an increase in regulatory T cells. The observed alterations of the patients' gut microbiota may also contribute to ileostomy's therapeutic effect. These data show that ileostomy induced significant clinical responses in patients with steroid-resistant GVHD along with a reduction of pro-inflammatory immune cells and changes of the intestinal microbiota. Ileostomy is a treatment option for steroid-resistant acute GVHD of the gastrointestinal tract that needs further validation in a prospective clinical trial.
Keywords: Graft-versus-host disease; Hematopoietic stem cell transplantation; Ileostomy-induced immune modulation; Intestinal adaptation; Intestinal microbiota; Refractory GVHD.
Conflict of interest statement
ATT has received lecture fees from Jazz Pharmaceuticals and travel subsidies from Neovii Biotech outside the submitted work. NKS received travel subsidies from MSD and Jazz, DWB received travel subsidies from Medac, all outside the submitted work. The other authors declare that they have no competing interests.
Figures
References
-
- MacMillan ML, Weisdorf DJ, Wagner JE, DeFor TE, Burns LJ, Ramsay NK, et al. Response of 443 patients to steroids as primary therapy for acute graft-versus-host disease: comparison of grading systems. Biol Blood Marrow Transplant. 2002;8(7):387–394. doi: 10.1053/bbmt.2002.v8.pm12171485. - DOI - PubMed
-
- Martin PJ, Rizzo JD, Wingard JR, Ballen K, Curtin PT, Cutler C, et al. First- and second-line systemic treatment of acute graft-versus-host disease: recommendations of the American Society of Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2012;18(8):1150–1163. doi: 10.1016/j.bbmt.2012.04.005. - DOI - PMC - PubMed
-
- Magenau JM, Goldstein SC, Peltier D, Soiffer RJ, Braun T, Pawarode A, Riwes MM, Kennel M, Antin JH, Cutler CS, Ho VT, Alyea EP, III, Parkin BL, Yanik GA, Choi SW, Lewis EC, Dinarello CA, Koreth J, Reddy P. alpha1-antitrypsin infusion for treatment of steroid-resistant acute graft-versus-host disease. Blood. 2018;131(12):1372–1379. doi: 10.1182/blood-2017-11-815746. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
