

MRI of the axial skeleton in spondyloarthritis: the many faces of new bone formation
- PMID: 31338670
- PMCID: PMC6650523
- DOI: 10.1186/s13244-019-0752-4
MRI of the axial skeleton in spondyloarthritis: the many faces of new bone formation
Abstract
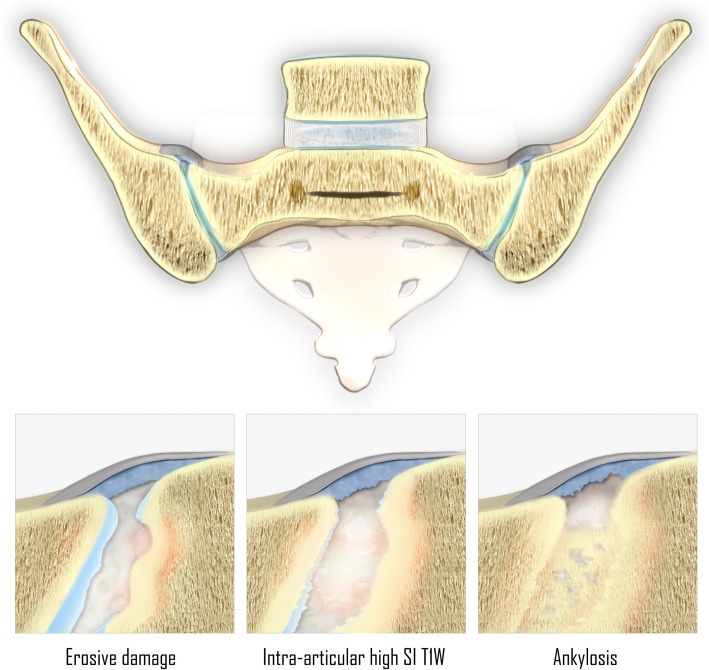
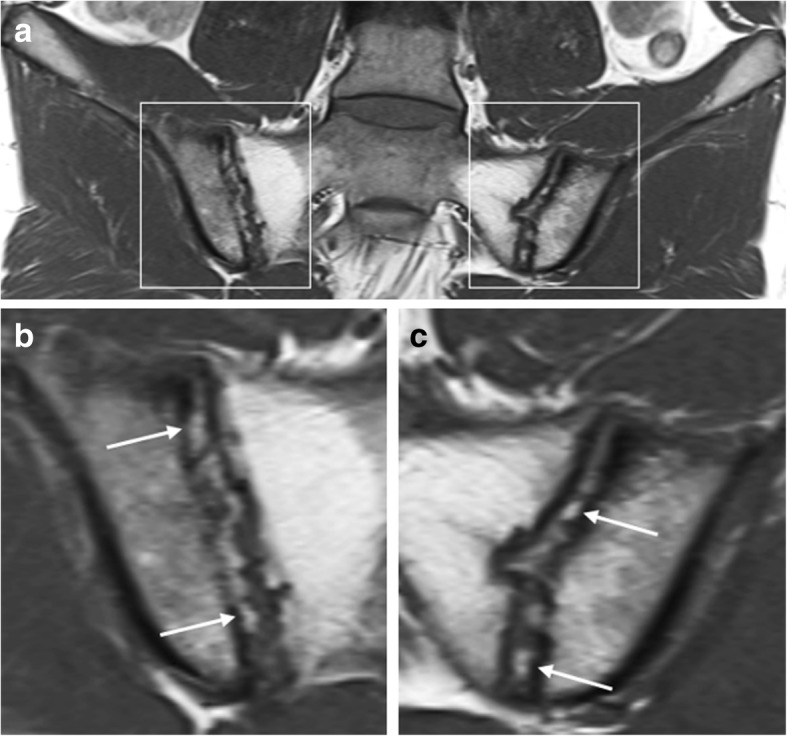
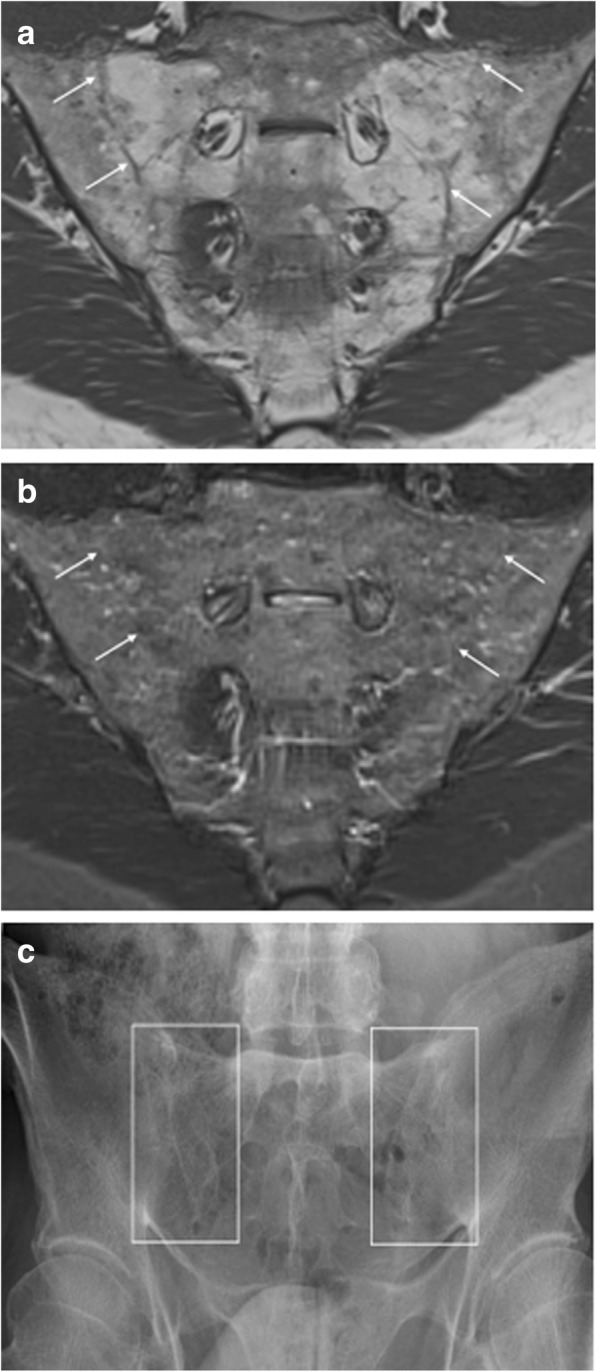
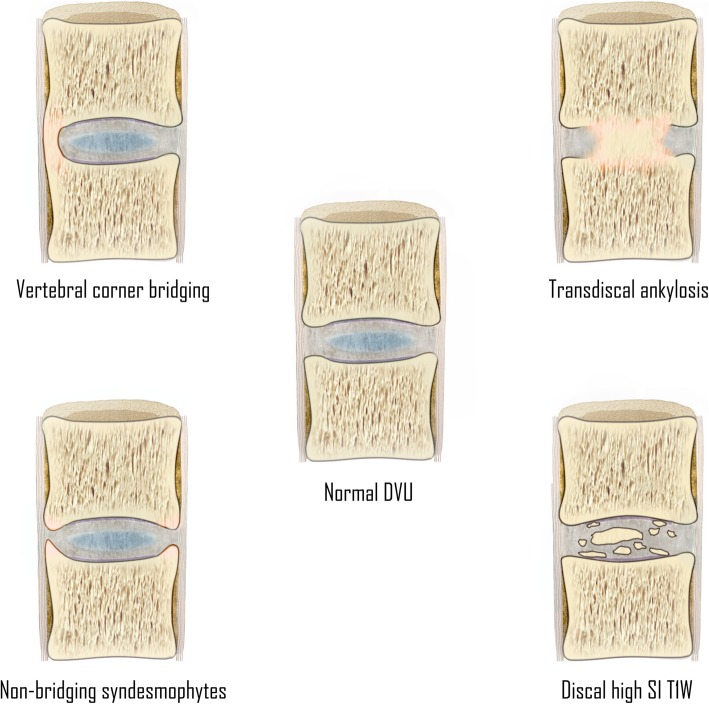
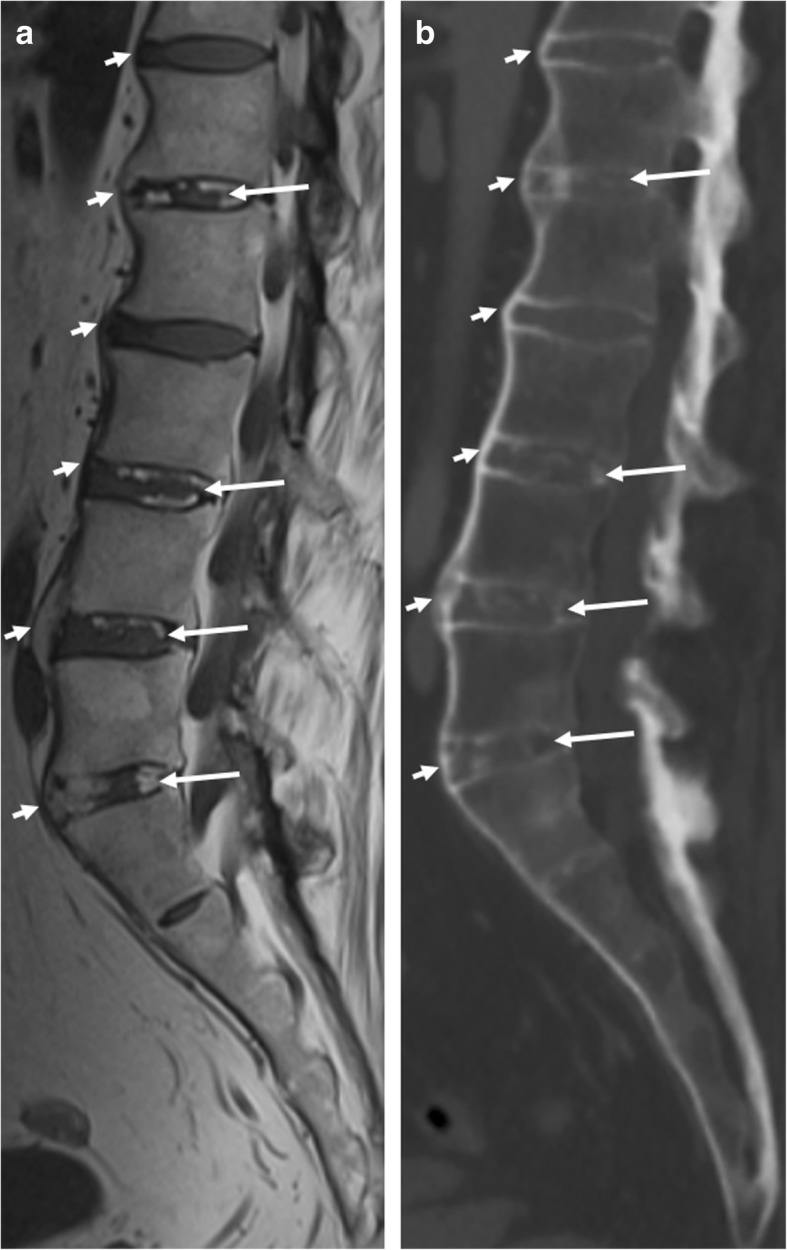
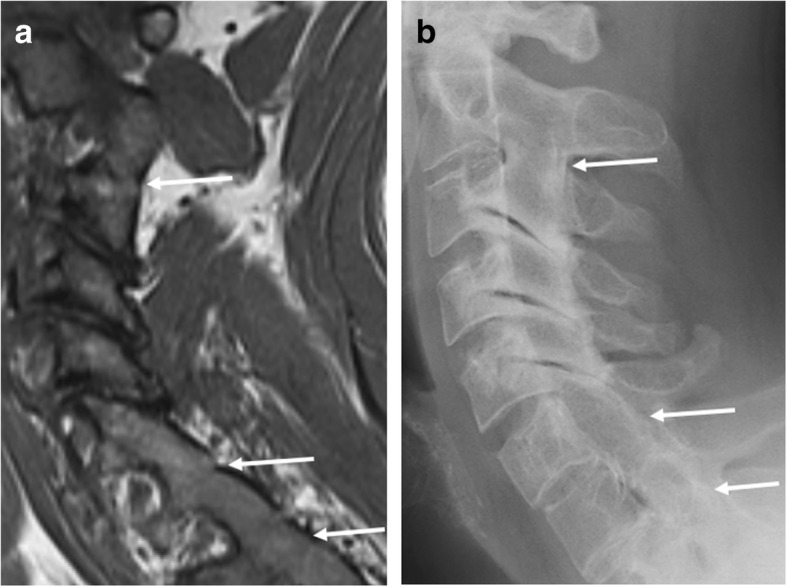
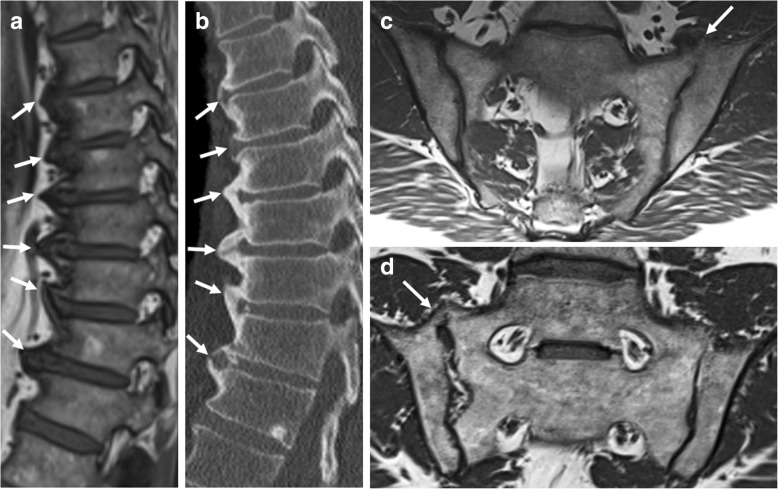
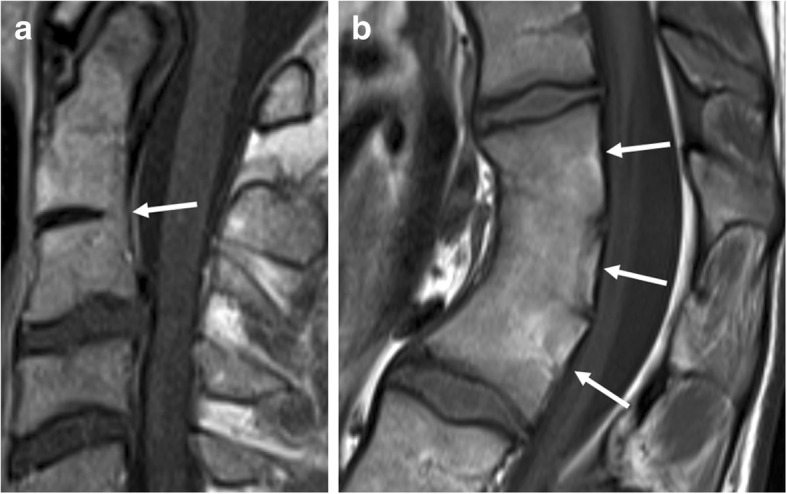
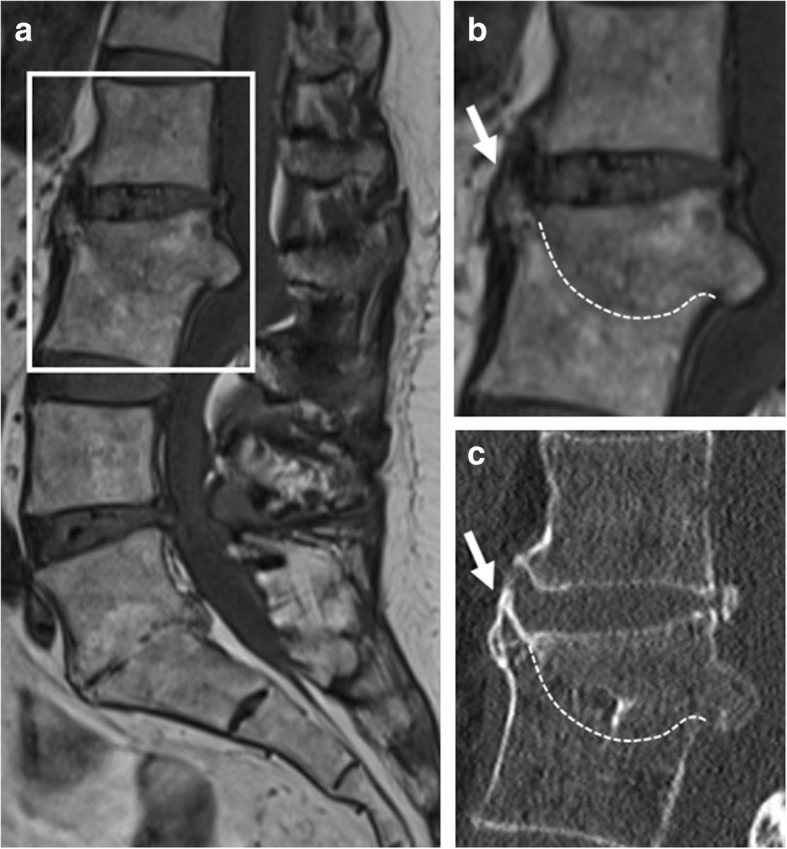
Spondyloarthritis has two hallmark features: active inflammation and structural lesions with new bone formation. MRI is well suited to assess active inflammation, but there is increasing interest in the role of structural lesions at MRI. Recent MRI studies have examined the established features of new bone formation and demonstrated some novel features which show diagnostic value and might even have potential as possible markers of disease progression. Although MRI is not the first imaging modality that comes into mind for assessment of bony changes, these features of new bone formation can be detected on MRI-if one knows how to recognize them. This review illustrates the MRI features of new bone formation and addresses possible pitfalls.
Keywords: Ankylosis; Magnetic resonance imaging; Sacroiliac joint; Spine; Spondyloarthritis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ward MM, Deodhar A, Akl EA, et al. American College Of Rheumatology/Spondylitis Association of America/Spondyloarthritis research and treatment network 2015 recommendations for the treatment of ankylosing spondylitis and non-radiographic axial spondyloarthritis. Arthritis Rheumatol. 2016;68:282–298. doi: 10.1002/art.39298. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
