

Atrophic Dermatofibroma: A Comprehensive Literature Review
- PMID: 31338755
- PMCID: PMC6704206
- DOI: 10.1007/s13555-019-0309-y
Atrophic Dermatofibroma: A Comprehensive Literature Review
Abstract
Introduction: An atrophic dermatofibroma is a benign fibrohistiocytic neoplasm. It typically presents as an asymptomatic patch with a depressed central area.
Methods: The PubMed database was used to search the following words: atrophic, dermatofibroma, elastic and fibers. The relevant papers and their references generated by the search were reviewed. Images of the clinical and pathological features of two patients with an atrophic dermatofibroma are presented. In addition, a comprehensive review of the characteristics of this unique dermatofibroma is provided.
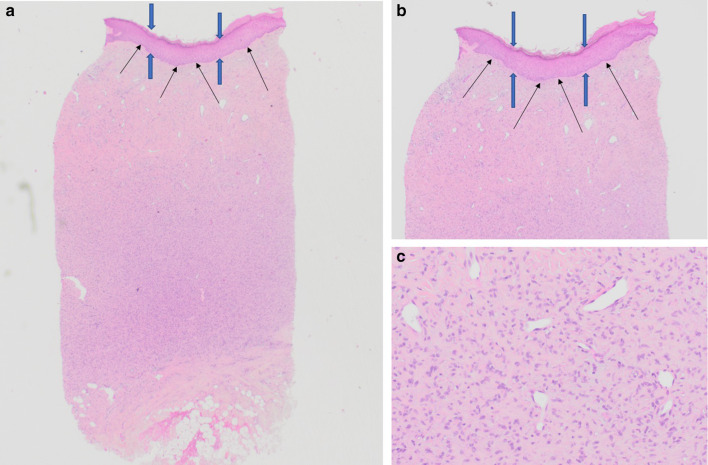
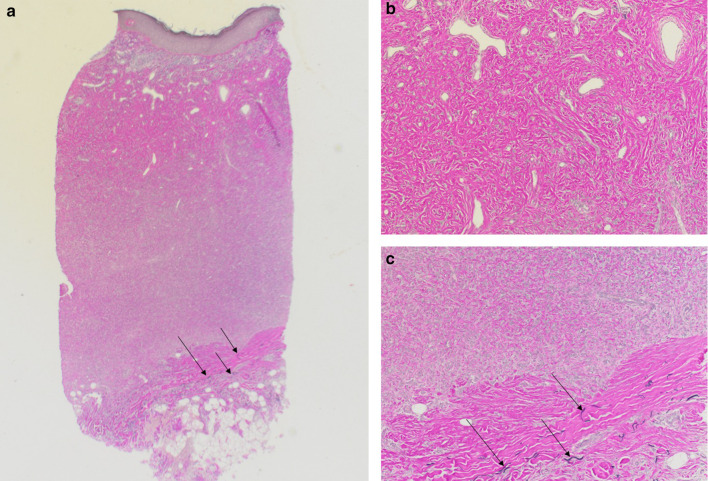
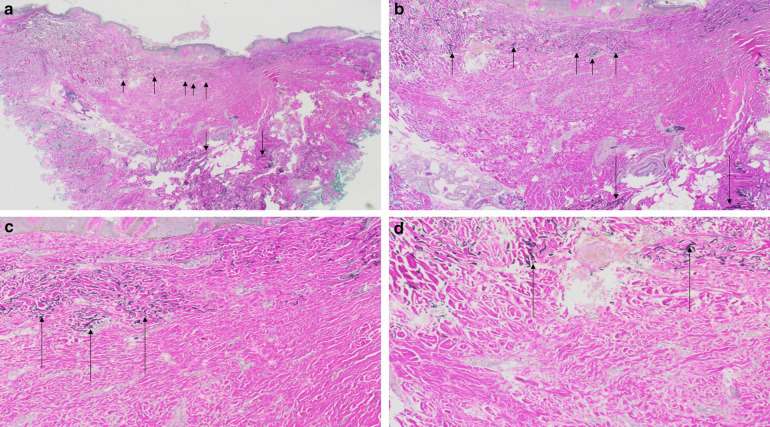
Results: An atrophic dermatofibroma has been reported in 102 patients: 53 women, 11 men and 38 individuals whose gender was not provided. It typically appeared as an asymptomatic solitary patch with a central umbilication-most commonly on the shoulder or lower extremity or back-of women aged 48 years or older. Dermoscopy typically showed white scar-like patches; a patchy pigment network was also noted in some lesions. The pathology of an atrophic dermatofibroma has the same features that can be observed in a common fibrous dermatofibroma; there is acanthosis, basal layer hyperpigmentation, and induction of basal cell carcinoma-like features, hair follicle formation or sebaceous hyperplasia in the epidermis and a proliferation of spindle-shaped fibroblasts in the dermis. However, atrophic dermatofibromas also demonstrate depression of the central surface and thinning of the dermis; in many cases, the dermal atrophy is at least 50%. Elastic fibers are either decreased or absent. Similar to non-atrophic dermatofibromas, the immunoperoxidase profile of atrophic dermatofibromas is factor XIIIa-positive and cluster of differentiation 34 (CD34)-negative. The pathogenesis of atrophic dermatofibromas remains to be established.
Conclusion: An atrophic dermatofibroma is an uncommon benign variant of a dermatofibroma. The diagnosis can be suspected based on clinical features and dermatoscopic findings. A biopsy of the lesion will confirm the diagnosis. Periodic evaluation of the lesion site is a reasonable approach to the management of the residual tumor.
Keywords: Atrophic; Depression; Dermatofibroma; Dermoscopy; Elastic; Fibers; Fibroblast; Men; Umbilication; Women.
Conflict of interest statement
Philip R. Cohen, Christof P. Erickson and Antoanella Calame have nothing to disclose with regards to the publication of this article. Philip R. Cohen is a member of the journal’s Editorial Board
Figures



References
-
- Myers DJ, Fillman EP. Dermatofibroma. StatPearls. Treasure Island: StatPearls Publishing; 2018. p. 27.
-
- Beatrous SV, Riahi RR, Grisoli SB, Cohen PR. Associated conditions in patients with multiple dermatofibromas: case reports and literature review. Dermatol Online J. 2017;23(9):13030. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
