

Mortality Risk and Fine Particulate Air Pollution in a Large, Representative Cohort of U.S. Adults
- PMID: 31339350
- PMCID: PMC6792459
- DOI: 10.1289/EHP4438
Mortality Risk and Fine Particulate Air Pollution in a Large, Representative Cohort of U.S. Adults
Erratum in
-
Erratum: "Mortality Risk and Fine Particulate Air Pollution in a Large, Representative Cohort of U.S. Adults".Environ Health Perspect. 2019 Sep;127(9):99002. doi: 10.1289/EHP6182. Epub 2019 Sep 27. Environ Health Perspect. 2019. PMID: 31559854 Free PMC article. No abstract available.
Abstract
Background: Evidence indicates that air pollution contributes to cardiopulmonary mortality. There is ongoing debate regarding the size and shape of the pollution–mortality exposure–response relationship. There are also growing appeals for estimates of pollution–mortality relationships that use public data and are based on large, representative study cohorts.
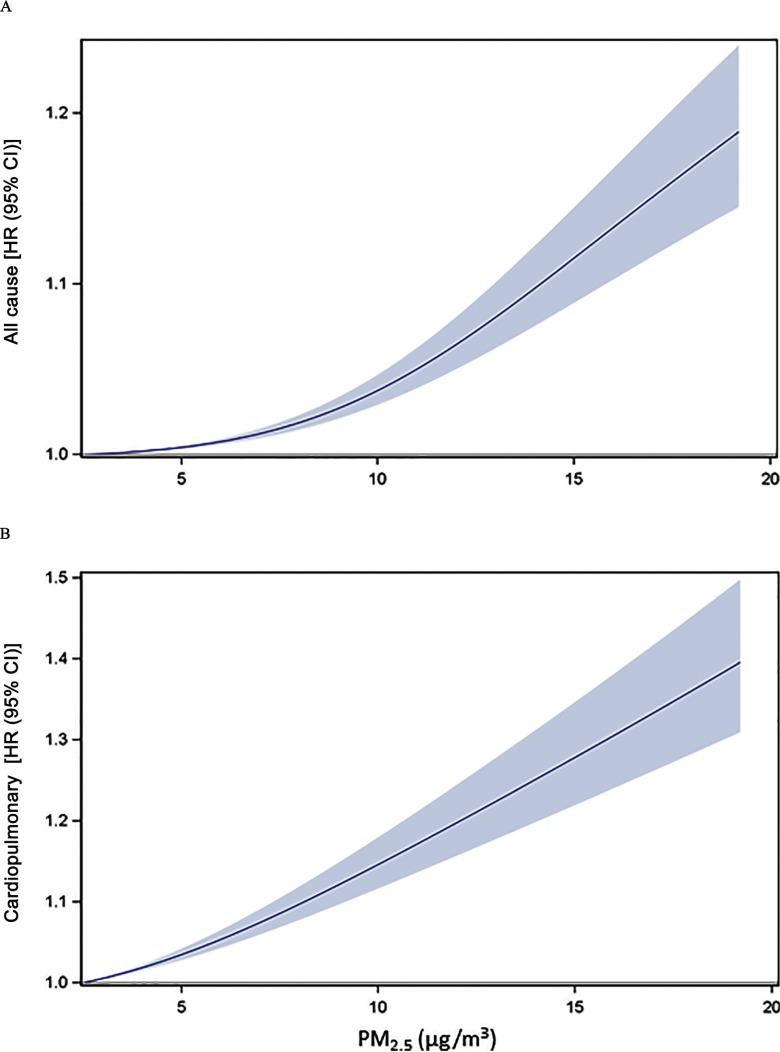
Objectives: Our goal was to evaluate fine particulate matter air pollution ([Formula: see text]) and mortality using a large cohort that is representative of the U.S. population and is based on public data. Additional objectives included exploring model sensitivity, evaluating relative effects across selected subgroups, and assessing the shape of the [Formula: see text]–mortality relationship.
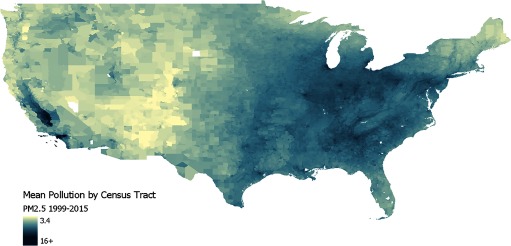
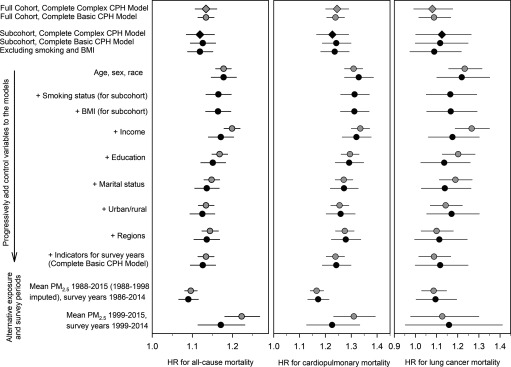
Methods: National Health Interview Surveys (1986–2014), with mortality linkage through 2015, were used to create a cohort of 1,599,329 U.S. adults and a subcohort with information on smoking and body mass index (BMI) of 635,539 adults. Data were linked with modeled ambient [Formula: see text] at the census-tract level. Cox proportional hazards models were used to estimate [Formula: see text]–mortality hazard ratios for all-cause and specific causes of death while controlling for individual risk factors and regional and urban versus rural differences. Sensitivity and subgroup analyses were conducted and the shape of the [Formula: see text]–mortality relationship was explored.
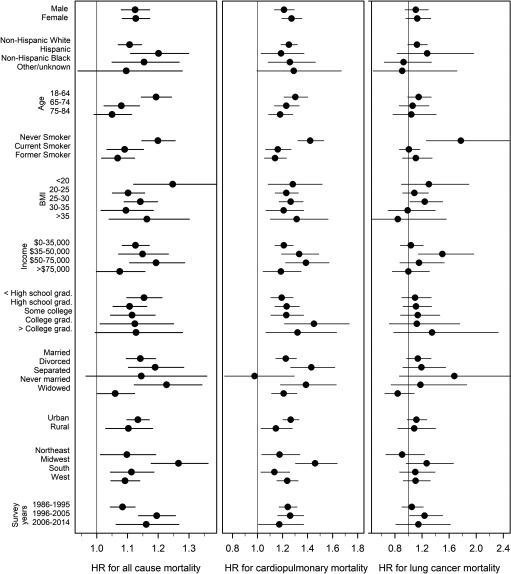
Results: Estimated mortality hazard ratios, per [Formula: see text] long-term exposure to [Formula: see text], were 1.12 (95% CI: 1.08, 1.15) for all-cause mortality, 1.23 (95% CI: 1.17, 1.29) for cardiopulmonary mortality, and 1.12 (95% CI: 1.00, 1.26) for lung cancer mortality. In general, [Formula: see text]–mortality associations were consistently positive for all-cause and cardiopulmonary mortality across key modeling choices and across subgroups of sex, age, race-ethnicity, income, education levels, and geographic regions.
Discussion: This large, nationwide, representative cohort of U.S. adults provides robust evidence that long-term [Formula: see text] exposure contributes to cardiopulmonary mortality risk. The ubiquitous and involuntary nature of exposures and the broadly observed effects across subpopulations underscore the public health importance of breathing clean air. https://doi.org/10.1289/EHP4438.
Figures
Comment in
-
Subtle but Potentially Serious: Long-Term Ambient Exposure and Risk of Cardiopulmonary Mortality.Environ Health Perspect. 2020 Feb;128(2):24001. doi: 10.1289/EHP6324. Epub 2020 Feb 26. Environ Health Perspect. 2020. PMID: 32101023 Free PMC article.
References
-
- Beelen R, Raaschou-Nielsen O, Stafoggia M, Andersen ZJ, Weinmayr G, Hoffmann B, et al. . 2014. Effects of long-term exposure to air pollution on natural-cause mortality: an analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 383(9919):785–795, PMID: 24332274, 10.1016/S0140-6736(13)62158-3. - DOI - PubMed
-
- Brook RD, Rajagopalan S, Pope CA III, Brook JR, Bhatnagar A, Diez-Roux AV, et al. . 2010. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 121(21):2331–2378, PMID: 20458016, 10.1161/CIR.0b013e3181dbece1. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
