

Demographics, Care Patterns, and Outcomes of Patients Admitted to Cardiac Intensive Care Units: The Critical Care Cardiology Trials Network Prospective North American Multicenter Registry of Cardiac Critical Illness
- PMID: 31339509
- PMCID: PMC6659157
- DOI: 10.1001/jamacardio.2019.2467
Demographics, Care Patterns, and Outcomes of Patients Admitted to Cardiac Intensive Care Units: The Critical Care Cardiology Trials Network Prospective North American Multicenter Registry of Cardiac Critical Illness
Abstract
Importance: Single-center and claims-based studies have described substantial changes in the landscape of care in the cardiac intensive care unit (CICU). Professional societies have recommended research to guide evidence-based CICU redesigns.
Objective: To characterize patients admitted to contemporary, advanced CICUs.
Design, setting, and participants: This study established the Critical Care Cardiology Trials Network (CCCTN), an investigator-initiated multicenter network of 16 advanced, tertiary CICUs in the United States and Canada. For 2 months in each CICU, data for consecutive admissions were submitted to the central data coordinating center (TIMI Study Group). The data were collected and analyzed between September 2017 and 2018.
Main outcomes and measures: Demographics, diagnoses, management, and outcomes.
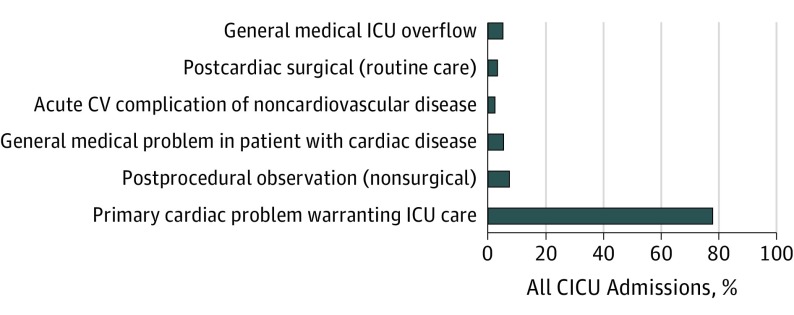
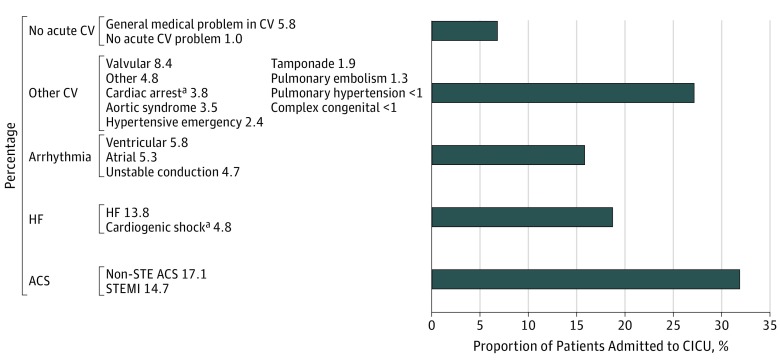
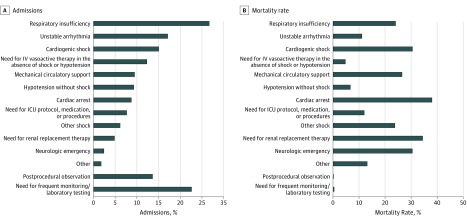
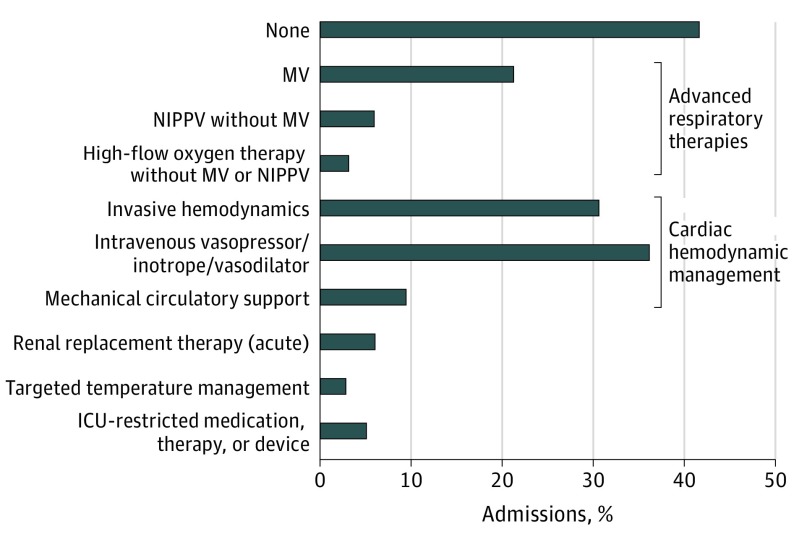
Results: Of 3049 participants, 1132 (37.1%) were women, 797 (31.4%) were individuals of color, and the median age was 65 years (25th and 75th percentiles, 55-75 years). Between September 2017 and September 2018, 3310 admissions were included, among which 2557 (77.3%) were for primary cardiac problems, 337 (10.2%) for postprocedural care, 253 (7.7%) for mixed general and cardiac problems, and 163 (4.9%) for overflow from general medical ICUs. When restricted to the initial 2 months of medical CICU admissions for each site, the primary analysis population included 3049 admissions with a high burden of noncardiovascular comorbidities. The top 2 CICU admission diagnoses were acute coronary syndrome (969 [31.8%]) and heart failure (567 [18.6%]); however, the proportion of acute coronary syndrome was highly variable across centers (15%-57%). The primary indications for CICU care included respiratory insufficiency (814 [26.7%]), shock (643 [21.1%]), unstable arrhythmia (521 [17.1%]), and cardiac arrest (265 [8.7%]). Advanced CICU therapies or monitoring were required for 1776 patients (58.2%), including intravenous vasoactive medications (1105 [36.2%]), invasive hemodynamic monitoring (938 [30.8%]), and mechanical ventilation (652 [21.4%]). The overall CICU mortality rate was 8.3% (95% CI, 7.3%-9.3%). The CICU indications that were associated with the highest mortality rates were cardiac arrest (101 [38.1%]), cardiogenic shock (140 [30.6%]), and the need for renal replacement therapy (51 [34.5%]). Notably, patients admitted solely for postprocedural observation or frequent monitoring had a mortality rate of 0.2% to 0.4%.
Conclusions and relevance: In a contemporary network of tertiary care CICUs, respiratory failure and shock predominated indications for admission and carried a poor prognosis. While patterns of practice varied considerably between centers, a substantial, low-risk population was identified. Multicenter collaborative networks, such as the CCCTN, could be used to help redesign cardiac critical care and to test new therapeutic strategies.
Conflict of interest statement
Figures
References
-
- Morrow DA, Fang JC, Fintel DJ, et al. ; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Council on Quality of Care and Outcomes Research . Evolution of critical care cardiology: transformation of the cardiovascular intensive care unit and the emerging need for new medical staffing and training models: a scientific statement from the American Heart Association. Circulation. 2012;126(11):1408-1428. doi: 10.1161/CIR.0b013e31826890b0 - DOI - PubMed
-
- Watson RA, Bohula EA, Gilliland TC, Sanchez PA, Berg DD, Morrow DA. Prospective registry of cardiac critical illness in a modern tertiary care cardiac intensive care unit [published online July 1, 2018]. Eur Heart J Acute Cardiovasc Care. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
